Thu, Jul 16, 2026
[Archive]
Volume 2, Issue 3 (Spring 2024)
CPR 2024, 2(3): 187-196 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hashem Varzi M R, Ghazanfari A. Comparing the Effectiveness of Short-term Intensive Dynamic Psychotherapy and Schema Therapy on
Perceived Stress in Patients With Hypertension. CPR 2024; 2 (3) :187-196
URL: http://cpr.mazums.ac.ir/article-1-118-en.html
URL: http://cpr.mazums.ac.ir/article-1-118-en.html



Department of Psychology, Faculty of Humanities, Shahrekord Branch, Islamic Azad University, Shahrekord, Iran.
Full-Text [PDF 780 kb]
(342 Downloads)
| Abstract (HTML) (1103 Views)
References
Full-Text: (348 Views)
Introduction
In recent years, cardiovascular diseases have become significantly prevalent worldwide. According to World Health Organization (WHO), more than 17.5 million deaths worldwide annually are caused by cardiovascular diseases [1]. Hypertension is among the leading risk factors for cardiovascular diseases. Hypertension accounts for a significant proportion of deaths in low- and middle-income societies [2]. Developing societies are twice as likely to suffer from hypertension as developed societies [3]. Studies conducted in Iran indicate a 23% prevalence of hypertension in individuals aged 30 to 35 years and a 50% prevalence in those over 55 years [4]. Based on these statistics, the WHO has developed an action plan to reduce hypertension by 25% by the end of 2025 [5].
The World Heart Federation defines blood pressure as the force exerted by blood against the walls of blood vessels as it circulates [5]. According to diagnostic criteria, elevated blood pressure becomes hypertension when measurements show >140 mm Hg (systolic) or >90 mm Hg (diastolic). Various factors are involved in increasing blood pressure. Stress is one of the main factors in the development of cardiovascular diseases and hypertension [6]. In stressful or threatening situations, visceral blood vessels constrict, triggering increased heart rate and elevated blood pressure [7]. According to research, stress is one of the significant factors in the increase in global mortality due to heart disease [8]. One of the factors that affects cardiovascular diseases is perceived stress [9].
Perceived stress refers to the body’s adaptive response to any demanding circumstance that requires physical, psychological, or emotional adjustment. According to studies, primary hypertension can be caused by psychological and stressful tensions [7]. In addition, hypertension and stress interact and affect people’s quality of life (QoL) [10]. Although medication is available for hypertensive patients, complementary non-pharmacological interventions remain essential for improving their QoL [11].
Schema therapy (ST) is one of the new and effective psychological treatment approaches for chronic problems, including hypertension [12]. Jeffrey Young invented ST in 1990, and it is used today as a psychological treatment—an effective therapeutic model for treating psychological disorders and a therapeutic style for treating chronic diseases. It integrates principles and concepts from several approaches, including cognitive-behavioral therapy, Gestalt therapy, and psychodynamic therapy. Young considers the goal of ST to increase adaptive responses to the environment to satisfy emotional needs and, as a result, improve mental health [13]. Zarei and Fooladvand investigated ST’s effectiveness on cardiovascular patients’ perceived stress in a study, and the results indicated a positive effect of this therapy on patients’ stress levels [14]. In another study, Nikan et al. reported the effectiveness of ST on stress in patients with cardiovascular diseases [15].
Another non-pharmacological approach effective in modulating psychological variables such as stress is intensive short-term dynamic psychotherapy (ISTDP). This approach has been developed and refined through the work of individuals such as Driessen et al. [16]. This approach focuses on individuals’ unconscious emotional conflicts so that they can understand and process their unconscious conflicts in the present moment without using defense mechanisms [17]. According to Freud, anxiety causes the formation of defense mechanisms in individuals, and these defense mechanisms are, in fact, ineffective strategies that lead to repression and failure to experience feelings and emotions. As a result, individuals become involved in psychological disorders, and their ability to face challenges decreases. Therefore, this approach attempts to enable individuals to experience anxiety without resistance [18]. Studies have shown the effectiveness of ISTDP in improving patients’ stress and anxiety [17, 19]. In a study, Amin Rostamkalai and Sadeghi [20] reported the effectiveness of ISTDP on self-management in patients with cardiovascular diseases.
Given the increasing incidence of hypertension in society, this study aimed to compare the effectiveness of ISTDP and ST on perceived stress in patients suffering from hypertension.
Materials and Methods
The present study was quasi-experimental, with a pre-test-post-test design and a control group. The research population included all hypertensive patients who sought care at comprehensive health service centers in Sari City, Iran, in 2023. The research sample included 45 people with hypertension, selected through purposive sampling. Clients with hypertension were referred to specialists by physicians working in health service centers. One hundred fifty-eight clients completed the perceived stress questionnaire (PSQ) with hypertension seeking care at Sari City’s comprehensive health service centers to collect data.
Among them, 45 people were selected based on scoring two standard deviations above the mean score on the life stress questionnaire and meeting other study inclusion criteria.
The inclusion criteria for the study were as follows: Diagnosis of hypertension, the experience of perceived stress, defined as a score two standard deviations above the mean on the PSQ, without using psychiatric medications such as venlafaxine or paroxetine, no history of addiction, or any psychiatric disorder.
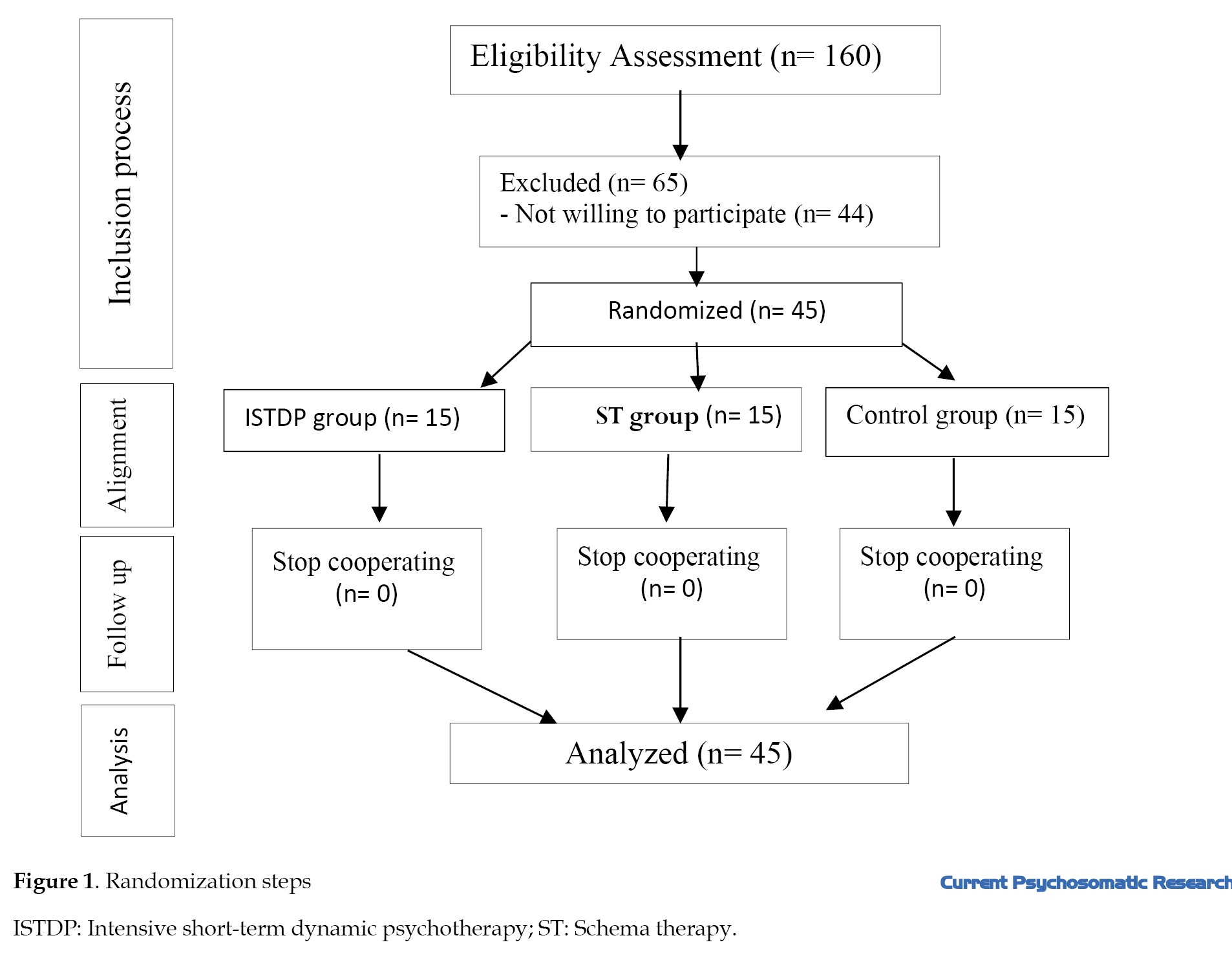
Participants were excluded if they withdrew consent, missed more than two sessions, experienced disease recurrence, or developed any physical illness during the intervention (Figure 1).
In recent years, cardiovascular diseases have become significantly prevalent worldwide. According to World Health Organization (WHO), more than 17.5 million deaths worldwide annually are caused by cardiovascular diseases [1]. Hypertension is among the leading risk factors for cardiovascular diseases. Hypertension accounts for a significant proportion of deaths in low- and middle-income societies [2]. Developing societies are twice as likely to suffer from hypertension as developed societies [3]. Studies conducted in Iran indicate a 23% prevalence of hypertension in individuals aged 30 to 35 years and a 50% prevalence in those over 55 years [4]. Based on these statistics, the WHO has developed an action plan to reduce hypertension by 25% by the end of 2025 [5].
The World Heart Federation defines blood pressure as the force exerted by blood against the walls of blood vessels as it circulates [5]. According to diagnostic criteria, elevated blood pressure becomes hypertension when measurements show >140 mm Hg (systolic) or >90 mm Hg (diastolic). Various factors are involved in increasing blood pressure. Stress is one of the main factors in the development of cardiovascular diseases and hypertension [6]. In stressful or threatening situations, visceral blood vessels constrict, triggering increased heart rate and elevated blood pressure [7]. According to research, stress is one of the significant factors in the increase in global mortality due to heart disease [8]. One of the factors that affects cardiovascular diseases is perceived stress [9].
Perceived stress refers to the body’s adaptive response to any demanding circumstance that requires physical, psychological, or emotional adjustment. According to studies, primary hypertension can be caused by psychological and stressful tensions [7]. In addition, hypertension and stress interact and affect people’s quality of life (QoL) [10]. Although medication is available for hypertensive patients, complementary non-pharmacological interventions remain essential for improving their QoL [11].
Schema therapy (ST) is one of the new and effective psychological treatment approaches for chronic problems, including hypertension [12]. Jeffrey Young invented ST in 1990, and it is used today as a psychological treatment—an effective therapeutic model for treating psychological disorders and a therapeutic style for treating chronic diseases. It integrates principles and concepts from several approaches, including cognitive-behavioral therapy, Gestalt therapy, and psychodynamic therapy. Young considers the goal of ST to increase adaptive responses to the environment to satisfy emotional needs and, as a result, improve mental health [13]. Zarei and Fooladvand investigated ST’s effectiveness on cardiovascular patients’ perceived stress in a study, and the results indicated a positive effect of this therapy on patients’ stress levels [14]. In another study, Nikan et al. reported the effectiveness of ST on stress in patients with cardiovascular diseases [15].
Another non-pharmacological approach effective in modulating psychological variables such as stress is intensive short-term dynamic psychotherapy (ISTDP). This approach has been developed and refined through the work of individuals such as Driessen et al. [16]. This approach focuses on individuals’ unconscious emotional conflicts so that they can understand and process their unconscious conflicts in the present moment without using defense mechanisms [17]. According to Freud, anxiety causes the formation of defense mechanisms in individuals, and these defense mechanisms are, in fact, ineffective strategies that lead to repression and failure to experience feelings and emotions. As a result, individuals become involved in psychological disorders, and their ability to face challenges decreases. Therefore, this approach attempts to enable individuals to experience anxiety without resistance [18]. Studies have shown the effectiveness of ISTDP in improving patients’ stress and anxiety [17, 19]. In a study, Amin Rostamkalai and Sadeghi [20] reported the effectiveness of ISTDP on self-management in patients with cardiovascular diseases.
Given the increasing incidence of hypertension in society, this study aimed to compare the effectiveness of ISTDP and ST on perceived stress in patients suffering from hypertension.
Materials and Methods
The present study was quasi-experimental, with a pre-test-post-test design and a control group. The research population included all hypertensive patients who sought care at comprehensive health service centers in Sari City, Iran, in 2023. The research sample included 45 people with hypertension, selected through purposive sampling. Clients with hypertension were referred to specialists by physicians working in health service centers. One hundred fifty-eight clients completed the perceived stress questionnaire (PSQ) with hypertension seeking care at Sari City’s comprehensive health service centers to collect data.
Among them, 45 people were selected based on scoring two standard deviations above the mean score on the life stress questionnaire and meeting other study inclusion criteria.
The inclusion criteria for the study were as follows: Diagnosis of hypertension, the experience of perceived stress, defined as a score two standard deviations above the mean on the PSQ, without using psychiatric medications such as venlafaxine or paroxetine, no history of addiction, or any psychiatric disorder.
Participants were excluded if they withdrew consent, missed more than two sessions, experienced disease recurrence, or developed any physical illness during the intervention (Figure 1).
A qualified clinical psychologist at the Sari City Counseling Center implemented clinical interventions. Due to ethical considerations, before executing the project, while obtaining written consent from the participants, they were reminded that the information received from each member would remain completely confidential and that each member could withdraw from the training course at any time wished.
A total of 45 participants were divided into three groups of 15. The first group received intervention type 1 (ST), and the second group received intervention type 2 (ISTDP). The third group, as a control group, did not receive any intervention, and no sample dropout occurred in any of the groups during the study.
ISTDP intervention sessions were conducted for the experimental group, consisting of eleven 90-minute sessions. Concurrently, the ST protocol was administered to another experimental group of patients, involving nine 120-minute sessions. The control group did not receive any intervention. The experimental and control groups completed the PSQ before and after implementing the psychological interventions.
SPSS software, version 26 was utilized for descriptive and inferential statistical data analysis. The significance level was set at 0.05. Repeated measures analysis of variance (MANOVA) followed by the Bonferroni post hoc test for pairwise comparisons was used to analyze the data. Before conducting the study, Mauchly’s test of sphericity for the assumption of sphericity, the Kolmogorov-Smirnov and Shapiro-Wilk tests for the normality of the data, and Levene’s test for the assumption of equality of variances were conducted.
Study measures
Demographic questionnaire included age, gender, education level, and employment status.
Cohen et al. (1983) developed the PSQ. The tool evaluates an individual’s subjective stress experience during the previous month, examining cognitive appraisals, emotional responses to stressful situations, and perceived ability to manage psychological pressures [21]. This scale has 14 items that are scored on a 4-point Likert scale (“never” to “very much”), and each item has a score between 0 and 4. A score above 36 demonstrates high perceived stress, and below 18 indicates low perceived stress. Saadat et al. [22] reported the reliability of the questionnaire using the Cronbach α method to be above 0.70. To calculate the validity of this scale, Cohen et al. calculated its correlation coefficient with symptomatology measures to be between 0.52 and 0.76 [21]. The construct validity coefficients of this questionnaire were calculated using simple correlation calculation with a researcher-made criterion question of 0.63, which was significant at the P<0.05 level [21]. Also, the Cronbach α coefficient in this study was 0.726.
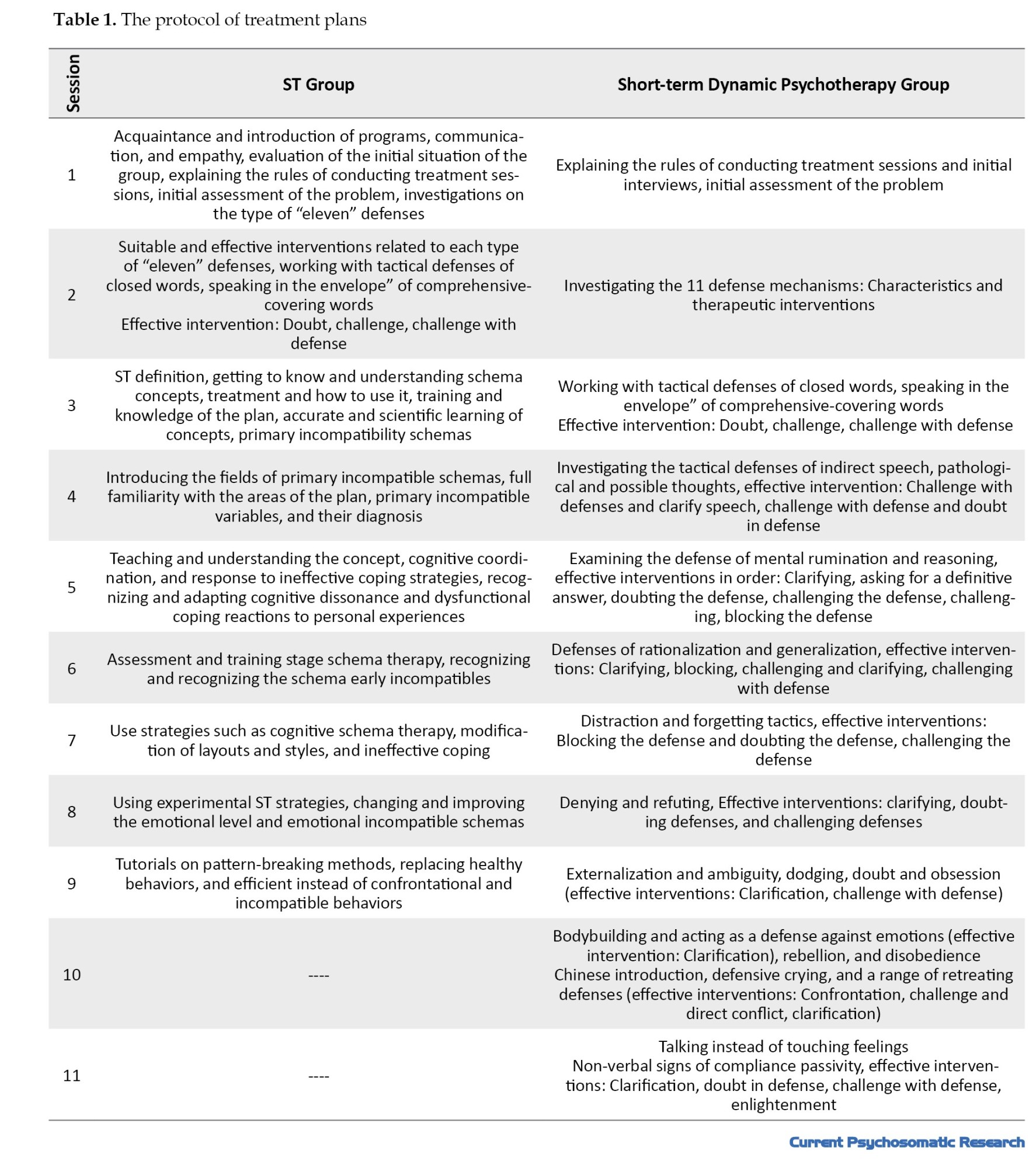
The protocol for the ISTDP intervention sessions consisted of eleven 90-minute sessions, which were implemented according to Davanlou’s dynamic psychotherapy manual (1995) [23]. Young et al. designed the ST intervention session protocol, including nine 120-minute sessions [24] (Table 1).
Results
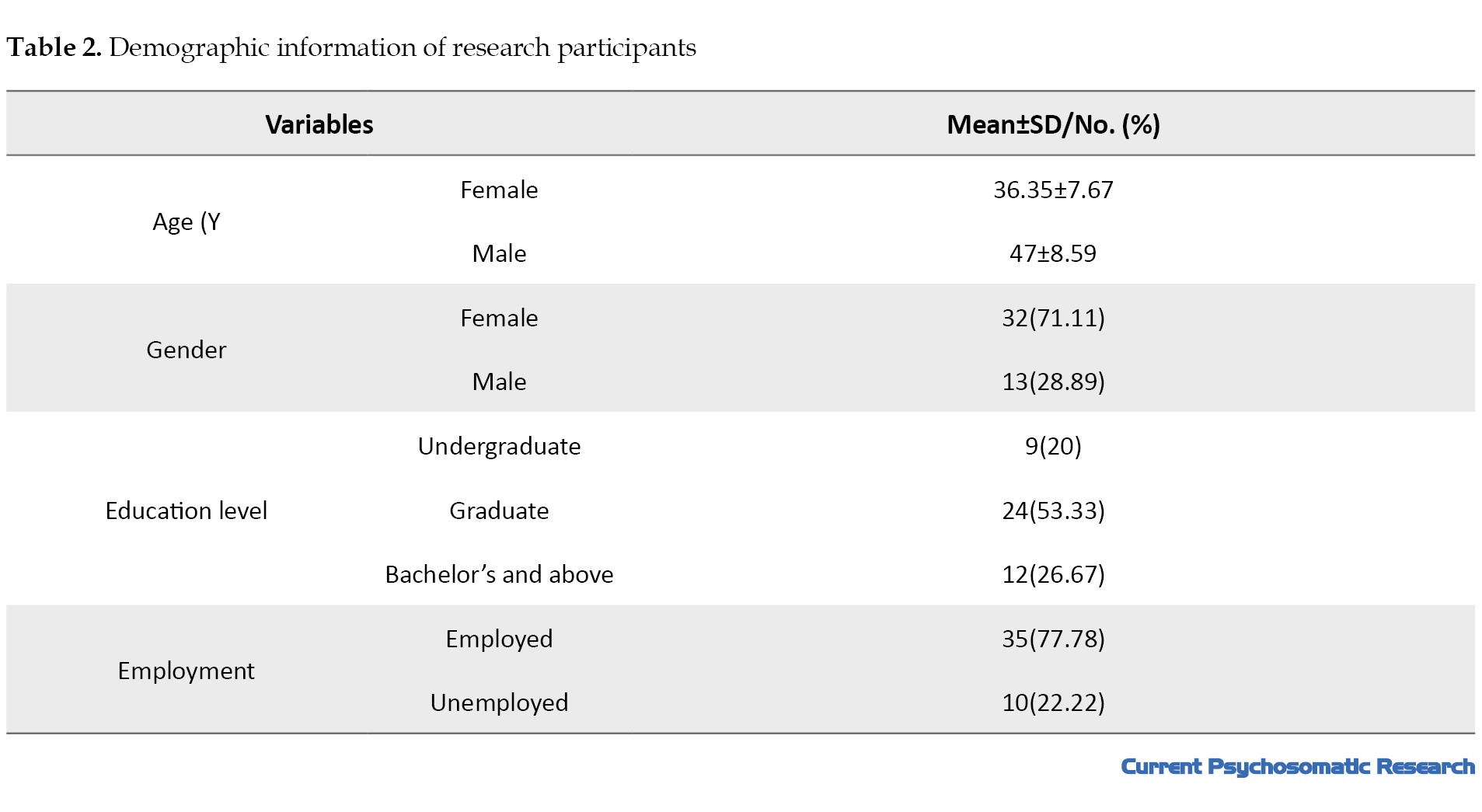
The Mean±SD age of the participants in the study was 36.35±7.67 years for women and about 47±8.59 years for men.
The first group consisted of 7 women and 8 men, while the second group had 3 women and 12 men. The control group included 5 women and 10 men. The age of participants in all three groups ranged from at least 20 years to a maximum of 55 years.
Regarding educational status, the first group had 7 women with diplomas, 4 men with bachelor’s degrees, and 4 with master’s degrees. The second group comprised 3 women with diplomas, 6 men with bachelor’s degrees, and 6 with master’s degrees. In the control group, there were 3 women with diplomas, 2 women with associate degrees, 6 men with bachelor’s degrees, and 4 men with master’s degrees. The first group included 10 employed individuals and 5 homemakers regarding employment status. The second group had 12 employed individuals and 3 homemakers, while the control group included 12 employed individuals and 3 homemakers. There was no significant difference between the three groups.
A summary of the demographic information of the study participants is reported in Table 2.
The normality of the data was confirmed across all study variables using the Kolmogorov-Smirnov test (P>0.001). Through Levene’s test, statistical analyses confirmed equal variance between experimental and control groups at all assessment points (pre-test, post-test, and follow-up).
However, Mauchly’s test revealed violations of sphericity assumptions in the covariance matrix, requiring the application of the Greenhouse-Geisser correction. Subsequent repeated measures MANOVA analysis yielded two key findings. First, a statistically significant between-group effect emerged for perceived stress, indicating differential outcomes among the study conditions. Second, a significant within-group time effect was observed, demonstrating measurable changes in variable means across the three assessment periods from baseline through follow-up. Table 3 shows the measures of central tendency and variability of the scores of the research variables in the two experimental and control groups.
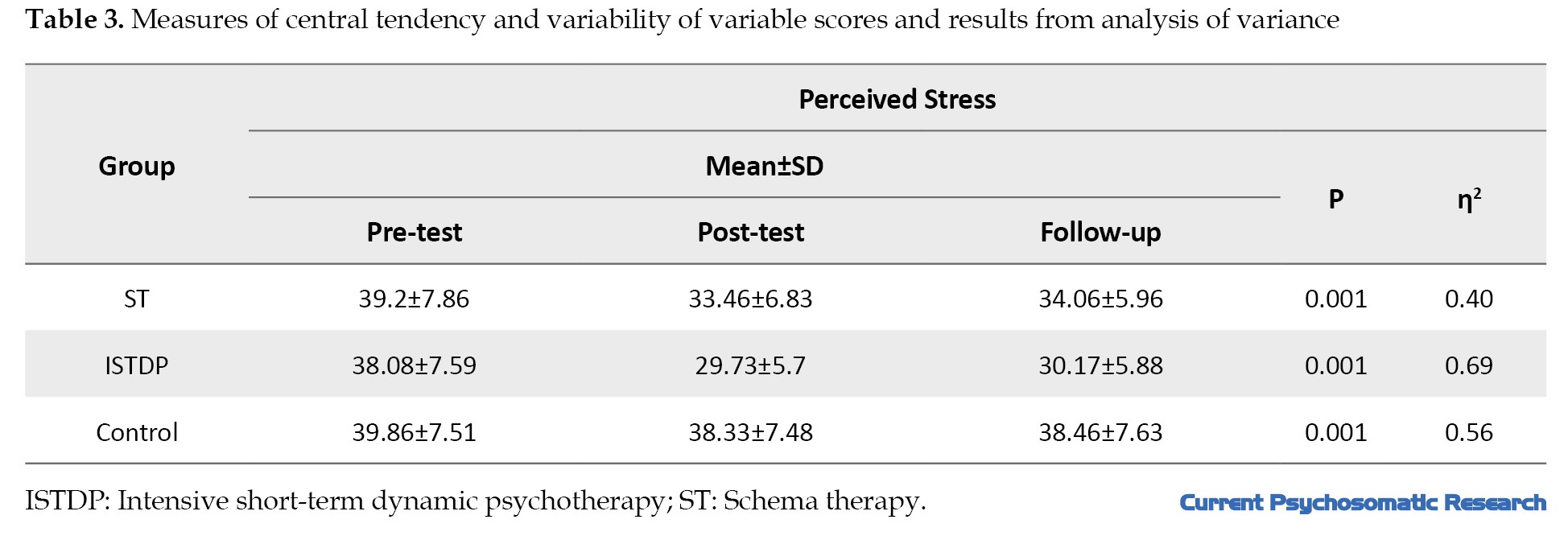
The results of the analysis of variance for the within-group (time) and between-group (group) factors are significant (Table 3).
The results presented in Table 2 show that, as opposed to the control group, perceived stress in both the ST and dynamic psychotherapy groups in the post-test was lower than in the pre-test (P<0.001). Moreover, the comparison of the two experimental groups showed that the score of the perceived stress variable in the ST and dynamic psychotherapy groups was significantly different from each other (P<0.001). Thus, dynamic psychotherapy had a greater effect on reducing perceived stress than schema therapy.
Changes in the experimental group over time in Table 4 indicate that the perceived stress variable was significant in both ST and dynamic psychotherapy groups in the post-test compared to the pre-test (P<0.001).
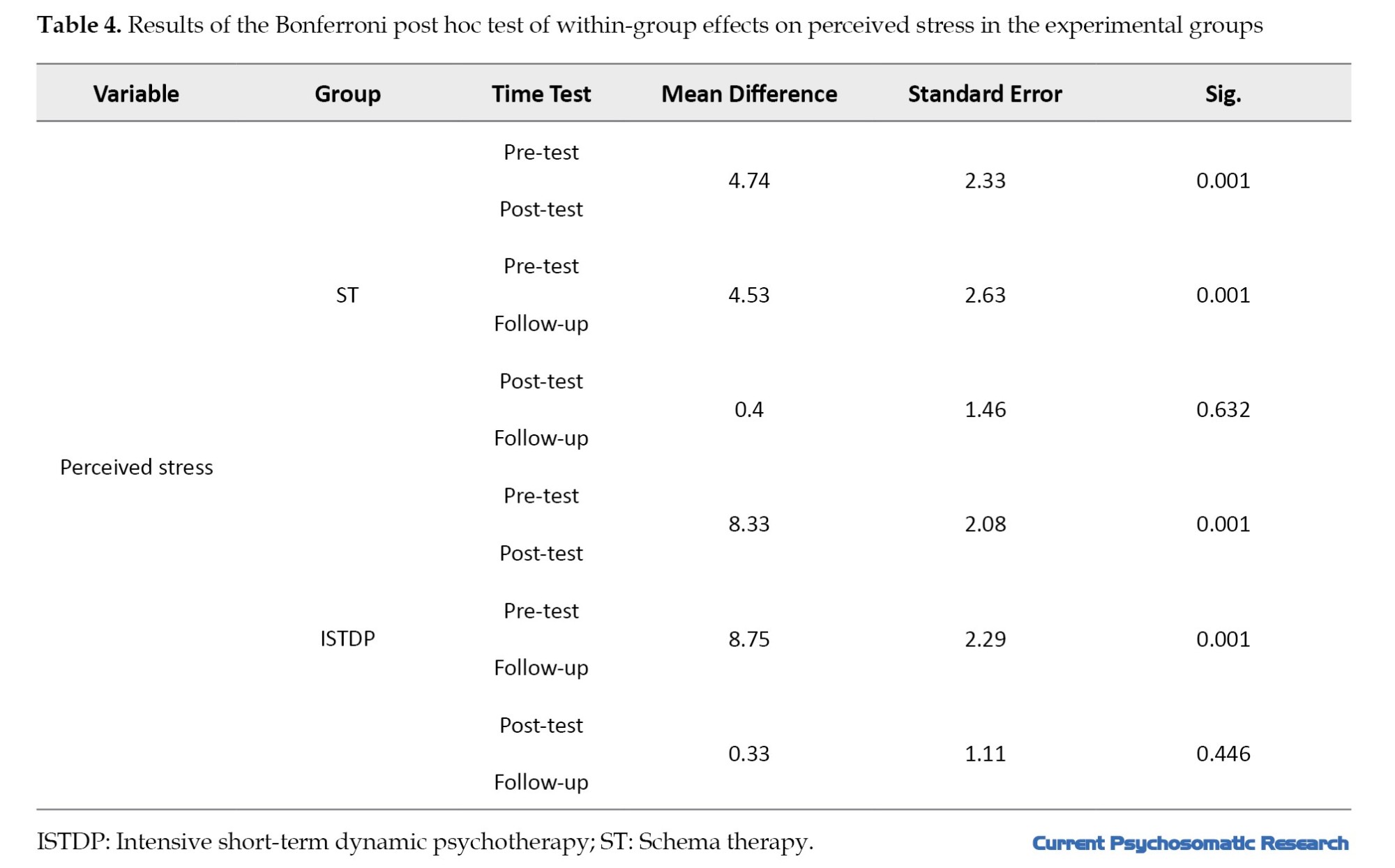
Also, a significant difference was observed in both follow-up stages compared to the pre-test (P<0.001). Still, in the follow-up stage, no significant difference was observed compared to the post-test (P>0.001), which means that the therapeutic effects of both treatments are durable.
Discussion
This study compared the efficacy of ISTDP and ST in reducing perceived stress among hypertensive patients. The findings demonstrate that ISTDP and ST are significantly more effective than the control condition in alleviating perceived stress, with treatment benefits persisting at follow-up assessments. Furthermore, a direct comparison between the two therapeutic approaches revealed that ISTDP produced superior stress-reduction outcomes compared to ST in this patient population. Regarding the effectiveness of ST on perceived stress in patients with hypertension, it should be acknowledged that this finding was consistent with the research of Zarei and Fooladvand [14], Mohammadi et al. [25], Hemmati Sabet et al. [26], Talayry and Bavi [27], and Kazemiani and Amiri [28].
ST allows patients to better adapt to current circumstances by identifying dysfunctional mental patterns and creating more adaptive responses to stressful situations and experienced stress. Schemas are a collection of memories, beliefs, emotions, and physical sensations that are relatively stable and can trigger stress in patients. According to this perspective, schemas are associated with unmet basic needs, and specific situations can activate them. If a schema is activated, it attacks the individual’s current awareness, leading to psychological disturbance; therefore, effective ST strategies can mitigate the cognitive damage of perceived stress in patients suffering from hypertension by breaking negative repetitive patterns and with the help of the principle of cognitive dissonance [14].
Regarding the effectiveness of ISTDP on perceived stress in patients with hypertension, it should be acknowledged that there was no consistent research to explain this finding, and the current study is considered innovative in its own right.
According to the principles of the ISTDP approach, anxiety occurs as a result of unaccepted emotions and thoughts, and the individual resorts to defense mechanisms to escape anxiety. This approach emphasizes identifying the distinct physical symptoms of emotions and guiding the individual toward the experience of emotions and physical symptoms associated with anxiety. In this way, this therapeutic approach helps to understand the dynamic pathological forces and causes of patients’ problems and assists them in resolving intrapersonal conflict.
As a result, this approach accepts emotions and provides a platform for their proper expression and discharge. Minimizing the use of maladaptive defense mechanisms facilitates psychological peace for the individual. Accordingly, identifying and experiencing stress effectively in cardiac patients significantly helps them to regulate and manage their current problems, and this improves the mental health of patients by building their capacity, removing defenses, and expressing unexpressed emotions and feelings [29].
Conclusion
This study demonstrates the efficacy of ST and ISTDP in reducing perceived stress among hypertensive patients. Future research should expand this investigation by exploring additional psychological variables in this population. Furthermore, implementing specialized training programs in these therapeutic approaches for clinicians and healthcare providers could enhance treatment quality and patient care outcomes.
Study limitations
The limitations of the article include a few research studies related to the topic of the article and the purposive sampling, which makes the generalizability of the results biased.
Study suggestions
It is suggested that future research use random sampling and control for the effects of confounding variables such as financial conditions. This research should be conducted on other exceptional disease groups, such as heart and diabetic patients and other diseases.
Ethical Considerations
Compliance with ethical guidelines
Patients were fully assured that their information would remain confidential and that they were allowed to withdraw from the trial if they did not consent. An attempt was made to keep the control group status constant until the end of the study.
This research has been approved by the Ethics Committee of Shahr-e-Kord Branch, Islamic Azad University, Shahr-e-Kord, Iran (Code: IR.IAU.SHK.REC.1402.144) and was registered by the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: IRCT20240505061653N1).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Review and writing of the final draft: Mahmoud Reza Hashem Varzi; Project supervision and management: Ahmad Ghazanfari; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their gratitude to all the participants in this study who helped us conduct this research.
A total of 45 participants were divided into three groups of 15. The first group received intervention type 1 (ST), and the second group received intervention type 2 (ISTDP). The third group, as a control group, did not receive any intervention, and no sample dropout occurred in any of the groups during the study.
ISTDP intervention sessions were conducted for the experimental group, consisting of eleven 90-minute sessions. Concurrently, the ST protocol was administered to another experimental group of patients, involving nine 120-minute sessions. The control group did not receive any intervention. The experimental and control groups completed the PSQ before and after implementing the psychological interventions.
SPSS software, version 26 was utilized for descriptive and inferential statistical data analysis. The significance level was set at 0.05. Repeated measures analysis of variance (MANOVA) followed by the Bonferroni post hoc test for pairwise comparisons was used to analyze the data. Before conducting the study, Mauchly’s test of sphericity for the assumption of sphericity, the Kolmogorov-Smirnov and Shapiro-Wilk tests for the normality of the data, and Levene’s test for the assumption of equality of variances were conducted.
Study measures
Demographic questionnaire included age, gender, education level, and employment status.
Cohen et al. (1983) developed the PSQ. The tool evaluates an individual’s subjective stress experience during the previous month, examining cognitive appraisals, emotional responses to stressful situations, and perceived ability to manage psychological pressures [21]. This scale has 14 items that are scored on a 4-point Likert scale (“never” to “very much”), and each item has a score between 0 and 4. A score above 36 demonstrates high perceived stress, and below 18 indicates low perceived stress. Saadat et al. [22] reported the reliability of the questionnaire using the Cronbach α method to be above 0.70. To calculate the validity of this scale, Cohen et al. calculated its correlation coefficient with symptomatology measures to be between 0.52 and 0.76 [21]. The construct validity coefficients of this questionnaire were calculated using simple correlation calculation with a researcher-made criterion question of 0.63, which was significant at the P<0.05 level [21]. Also, the Cronbach α coefficient in this study was 0.726.
The protocol for the ISTDP intervention sessions consisted of eleven 90-minute sessions, which were implemented according to Davanlou’s dynamic psychotherapy manual (1995) [23]. Young et al. designed the ST intervention session protocol, including nine 120-minute sessions [24] (Table 1).
Results
The Mean±SD age of the participants in the study was 36.35±7.67 years for women and about 47±8.59 years for men.
The first group consisted of 7 women and 8 men, while the second group had 3 women and 12 men. The control group included 5 women and 10 men. The age of participants in all three groups ranged from at least 20 years to a maximum of 55 years.
Regarding educational status, the first group had 7 women with diplomas, 4 men with bachelor’s degrees, and 4 with master’s degrees. The second group comprised 3 women with diplomas, 6 men with bachelor’s degrees, and 6 with master’s degrees. In the control group, there were 3 women with diplomas, 2 women with associate degrees, 6 men with bachelor’s degrees, and 4 men with master’s degrees. The first group included 10 employed individuals and 5 homemakers regarding employment status. The second group had 12 employed individuals and 3 homemakers, while the control group included 12 employed individuals and 3 homemakers. There was no significant difference between the three groups.
A summary of the demographic information of the study participants is reported in Table 2.
The normality of the data was confirmed across all study variables using the Kolmogorov-Smirnov test (P>0.001). Through Levene’s test, statistical analyses confirmed equal variance between experimental and control groups at all assessment points (pre-test, post-test, and follow-up).
However, Mauchly’s test revealed violations of sphericity assumptions in the covariance matrix, requiring the application of the Greenhouse-Geisser correction. Subsequent repeated measures MANOVA analysis yielded two key findings. First, a statistically significant between-group effect emerged for perceived stress, indicating differential outcomes among the study conditions. Second, a significant within-group time effect was observed, demonstrating measurable changes in variable means across the three assessment periods from baseline through follow-up. Table 3 shows the measures of central tendency and variability of the scores of the research variables in the two experimental and control groups.
The results of the analysis of variance for the within-group (time) and between-group (group) factors are significant (Table 3).
The results presented in Table 2 show that, as opposed to the control group, perceived stress in both the ST and dynamic psychotherapy groups in the post-test was lower than in the pre-test (P<0.001). Moreover, the comparison of the two experimental groups showed that the score of the perceived stress variable in the ST and dynamic psychotherapy groups was significantly different from each other (P<0.001). Thus, dynamic psychotherapy had a greater effect on reducing perceived stress than schema therapy.
Changes in the experimental group over time in Table 4 indicate that the perceived stress variable was significant in both ST and dynamic psychotherapy groups in the post-test compared to the pre-test (P<0.001).
Also, a significant difference was observed in both follow-up stages compared to the pre-test (P<0.001). Still, in the follow-up stage, no significant difference was observed compared to the post-test (P>0.001), which means that the therapeutic effects of both treatments are durable.
Discussion
This study compared the efficacy of ISTDP and ST in reducing perceived stress among hypertensive patients. The findings demonstrate that ISTDP and ST are significantly more effective than the control condition in alleviating perceived stress, with treatment benefits persisting at follow-up assessments. Furthermore, a direct comparison between the two therapeutic approaches revealed that ISTDP produced superior stress-reduction outcomes compared to ST in this patient population. Regarding the effectiveness of ST on perceived stress in patients with hypertension, it should be acknowledged that this finding was consistent with the research of Zarei and Fooladvand [14], Mohammadi et al. [25], Hemmati Sabet et al. [26], Talayry and Bavi [27], and Kazemiani and Amiri [28].
ST allows patients to better adapt to current circumstances by identifying dysfunctional mental patterns and creating more adaptive responses to stressful situations and experienced stress. Schemas are a collection of memories, beliefs, emotions, and physical sensations that are relatively stable and can trigger stress in patients. According to this perspective, schemas are associated with unmet basic needs, and specific situations can activate them. If a schema is activated, it attacks the individual’s current awareness, leading to psychological disturbance; therefore, effective ST strategies can mitigate the cognitive damage of perceived stress in patients suffering from hypertension by breaking negative repetitive patterns and with the help of the principle of cognitive dissonance [14].
Regarding the effectiveness of ISTDP on perceived stress in patients with hypertension, it should be acknowledged that there was no consistent research to explain this finding, and the current study is considered innovative in its own right.
According to the principles of the ISTDP approach, anxiety occurs as a result of unaccepted emotions and thoughts, and the individual resorts to defense mechanisms to escape anxiety. This approach emphasizes identifying the distinct physical symptoms of emotions and guiding the individual toward the experience of emotions and physical symptoms associated with anxiety. In this way, this therapeutic approach helps to understand the dynamic pathological forces and causes of patients’ problems and assists them in resolving intrapersonal conflict.
As a result, this approach accepts emotions and provides a platform for their proper expression and discharge. Minimizing the use of maladaptive defense mechanisms facilitates psychological peace for the individual. Accordingly, identifying and experiencing stress effectively in cardiac patients significantly helps them to regulate and manage their current problems, and this improves the mental health of patients by building their capacity, removing defenses, and expressing unexpressed emotions and feelings [29].
Conclusion
This study demonstrates the efficacy of ST and ISTDP in reducing perceived stress among hypertensive patients. Future research should expand this investigation by exploring additional psychological variables in this population. Furthermore, implementing specialized training programs in these therapeutic approaches for clinicians and healthcare providers could enhance treatment quality and patient care outcomes.
Study limitations
The limitations of the article include a few research studies related to the topic of the article and the purposive sampling, which makes the generalizability of the results biased.
Study suggestions
It is suggested that future research use random sampling and control for the effects of confounding variables such as financial conditions. This research should be conducted on other exceptional disease groups, such as heart and diabetic patients and other diseases.
Ethical Considerations
Compliance with ethical guidelines
Patients were fully assured that their information would remain confidential and that they were allowed to withdraw from the trial if they did not consent. An attempt was made to keep the control group status constant until the end of the study.
This research has been approved by the Ethics Committee of Shahr-e-Kord Branch, Islamic Azad University, Shahr-e-Kord, Iran (Code: IR.IAU.SHK.REC.1402.144) and was registered by the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: IRCT20240505061653N1).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Review and writing of the final draft: Mahmoud Reza Hashem Varzi; Project supervision and management: Ahmad Ghazanfari; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their gratitude to all the participants in this study who helped us conduct this research.
References
- Huang H, Zou Y, Chi H. Quantitative assessment of the effects of chitosan intervention on blood pressure control. Drug Des Devel Ther. 2017 Dec 28;12:67-75. [DOI:10.2147/DDDT.S148064] [PMID]
- Choudhury KN, Mainuddin AK, Wahiduzzaman M, Islam SM. Serum lipid profile and its association with hypertension in Bangladesh. Vasc Health Risk Manag. 2014; 10:327-32.[DOI:10.2147/VHRM.S61019] [PMID]
- Shafi ST, Shafi T. A survey of hypertension prevalence, awareness, treatment, and control in health screening camps of rural central Punjab, Pakistan. J Epidemiol Glob Health. 2017; 7(2):135-40. [DOI:10.1016/j.jegh.2017.01.001] [PMID]
- Shamsi A, Dehghan Nayeri N, Esmaeili M. Living with Hypertension: A qualitative research. Int J Community Based Nurs Midwifery. 2017; 5(3):219-30. [PMID]
- Dzudie A, Rayner B, Ojji D, Schutte AE, Twagirumukiza M, Damasceno A, et al. Pascar task force on hypertension roadmap to achieve 25% hypertension control in Africa. Cardio J Afric. 2017; 13(1): 54-9. [DOI: 10.1016/j.gheart.2017.06.001]
- Li Z, Li Y, Chen L, Chen P, Hu Y. Prevalence of Depression in Patients With Hypertension: A systematic review and meta-analysis. Medicine (Baltimore). 2015; 94(31):e1317.[DOI:10.1097/MD.0000000000001317] [PMID]
- Heidaran F, Sajjadian I, Fathi M. [Effectiveness of hypnotherapy on the perceived stress and blood pressure in patients with primary hypertension (Persian)]. Med J Mashhad Univ Med Sci. 2017; 60(5):669-80. [DOI:10.22038/mjms.2017.10451]
- Blum CA, Borglund S, Parcells D. High-fidelity nursing simulation: Impact on student self-confidence and clinical competence. Int J Nurs Educ Scholarsh. 2010; 7:Article 18. [DOI:10.2202/1548-923X.2035] [PMID]
- Heydarian F, Sajjadian E, Fathi M. [The effectiveness of hypnotherapy on perceived stress and blood pressure in patients with primary hypertension (Persian)]. J Facult Med Mashhad Univ Med Sci. 2016; 60(5):669-80. [Link]
- Kazemikhabiri K, Ajzashokouhi M, Kharazmi OA, Bemanian MR. Evaluation of quality of urban life with emphasis on health; A case study in Mashhad city. Environ. Health Eng. Manag. 2018; 5(1):57-60. [DOI:10.15171/EHEM.2018.08]
- Blumenthal JA, Sherwood A, Smith PJ, Mabe S, Watkins L, Lin PH, et al. Lifestyle modification for resistant hypertension: The TRIUMPH randomized clinical trial. Am Heart J. 2015; 170(5):986-94.e5. [DOI:10.1016/j.ahj.2015.08.006] [PMID]
- Ahmadi F, Goodarzi K, Farrokhi N, Roozbahani M. [Comparison of the effectiveness of acceptance and commitment therapy and schema therapy on resilience among patients with cardiovascular disease: A pilot study (Persian)]. Salāmat-i ijtimāi. 2021; 8(4):18-29. [Link]
- Ghaderi D, Mojtabaei M, Hatami M. [Construction and validation of the early emotional needs scale based on Yang's schema therapy theory (Persian)]. Appl Psychol. 2022; 16(1):112-93. [DOI:10.52547/apsy.2021.222985.1106]
- Zarei S, Fooladvand Kh. [The effectiveness of schema therapy on perceived stress and negative affect in coronary heart patients (Persian)]. Knowl Res App Psy. 2023; 24(91):151-62. [Link]
- Nikan A, Torabi A, Mohseninasab Z, Bahadori A, Javanmard Z, Hosinirad M. [Comparing the effectiveness of schema therapy and cognitive therapy based on mindfulness on stress, resilience, emotion regulation and psychological well-being of cardiovascular patients (Persian)]. J Res Psychol Health. 2023; 17 (1):46-60. [Link]
- Driessen E, Cuijpers P, de Maat SC, Abbass AA, de Jonghe F, Dekker JJ. The efficacy of short-term psychodynamic psychotherapy for depression: a meta-analysis. Clin Psychol Rev. 2010; 30(1):25-36. [DOI: 10.1016/j.cpr.2009.08.010] [PMID]
- Hatami H, Mohammadi N, Hadian Fard H, Aflakseir A A. [The effectiveness of schema therapy (ST) and intensive short-term dynamic psychotherapy (ISTDP) for improving emotion regulation in Complex PTSD (CPTSD) (Persian)]. J Res Psychol Health. 2024; 18(3):4. [Link]
- Ghazagh M, Lotfi Kashani F, Vaziri S, Zareh H. [Comparison of the effectiveness of acceptance and commitment therapy and intensive short-term dynamic psychotherapy on attention and executive function of patients with lupus erythematosus: A quasi-experimental single-subject study (Persian)]. Razi J Med Sci. 2023; 30(2):132-44. [Link]
- Ahmadi F, Vatankhah Amjad F, Kazemi Rezaei A, Mohammadi S. [The effectiveness of Intensive Short-Term Dynamic Psychotherapy (ISTDP (in symptoms depression, anxiety, posttraumatic stress and guilt felling in Bereaved people from the disease COVID-19) (Persian)]. J Nurs Manage. 2021; 10 (3):69-81. [Link]
- Amin Rostamkalai S, Sadeghi J. The effectiveness of short-term psychodynamic therapy on psychological self-management and cognitive flexibility. J Psychol Dyn Mood Disord. 1403; 3(5):101-17. [DOI:10.61838/kman.pdmd.3.5.9]
- Cohen S, Kamarak T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983; 24(4):385-96.[DOI:10.2307/2136404]
- Saadat S, Asghari F, Jazayeri R. [The relationship between academic self-efficacy with perceived stress, coping strategies and perceived social support among students of University of Guilan (Persian)]. Iran J Med Educ. 2015; 15:67-78. [Link]
- Davanloo H. [Unlocking the unconscious selected articles by Habib Dovanloo (Persian)]. Tehran: Arjmand Publication; 2023. [Link]
- Young JE, Klosko JS, Weishaar ME. Schema therapy: A practitioner’s guide. New York: Guilford Press; 2006. [Link]
- Mohammadi G, Karbalaei Mohammad Migooni A, Malihialzakerini S, Kalhornia Golkar M. [Comparison of the effect of schema therapy and dialectical behavior therapy on lifestyle of women with coronary artery heart disease (Persian)]. Iran J Cardiovasc Nurs. 2021; 10(1):38-48. [Link]
- Hemmati Sabet A, Navabi Nejad S, Khalatbari J. [Compare of effectiveness schema therapy and group cognitive therapy to reduce depression, anxiety and perceived stress women (Persian)]. Shenakht J Psychol Psychiatry. 2016; 3(1):12-25.[Link]
- Talayry A, bavi S. [Comparison of the effectiveness of mindfulness-based stress reduction therapy and emotional schema therapy on perceived stress and distress tolerance of women undergoing drug treatment with psoriasis in Ahvaz city (Persian)]. Iran J Psychiatr Nurs. 2023; 11 (5):40-52. [DOI:10.22034/IJPN.11.5.40]
- Kazemaini E, Amiri M. The effectiveness of schema therapy on perceived stress in patients with hypertension attending: Schema therapy’s impact on perceived stress in hypertension management. Int J Body Mind Cult. 2024; 11(5):613-9. [DOI:10.22122/ijbmc.v11i5.765]
- Ahmadi F, Vatankhah Amjad F. [The effectiveness of Intensive Short-Term Dynamic Psychotherapy (ISTDP (in symptoms depression, anxiety, posttraumatic stress and guilt felling in Bereaved people from the disease COVID-19 (Persian)]. Faslnamah-i Mudiriyyat-i Parastari. 2021; 10(3):69-81. [Link]
Type of Study: Research |
Subject:
Psychology
Received: 2024/09/15 | Accepted: 2025/05/10 | Published: 2024/04/1
Received: 2024/09/15 | Accepted: 2025/05/10 | Published: 2024/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
