Wed, May 27, 2026
[Archive]
Volume 2, Issue 1 (Autumn 2023)
CPR 2023, 2(1): 65-72 |
Back to browse issues page


Research code: ۶۶۳۴۰
Ethics code: IR.MAZUMS.REC.332
Clinical trials code: IRCT20160619028528N7
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Salarian N, Elyasi F, Nasab N M, Hamzehgardeshi Z, Ebrahimi M E. The Effect of Abbreviated Online Counseling Based on Mindfulness on the Level of Distress of Women With Infertility Undergoing Assisted Reproductive Methods: A Study Protocol. CPR 2023; 2 (1) :65-72
URL: http://cpr.mazums.ac.ir/article-1-93-en.html
URL: http://cpr.mazums.ac.ir/article-1-93-en.html
Negin Salarian 

 , Forouzan Elyasi , Noraddin Mousavi Nasab , Zeinab Hamzehgardeshi , Mohammad Esmail Ebrahimi
, Forouzan Elyasi , Noraddin Mousavi Nasab , Zeinab Hamzehgardeshi , Mohammad Esmail Ebrahimi
, Forouzan Elyasi , Noraddin Mousavi Nasab , Zeinab Hamzehgardeshi , Mohammad Esmail Ebrahimi
Student Research Committee, Mazandaran University of Medical Sciences, Sari, Iran.
Full-Text [PDF 770 kb]
(939 Downloads)
| Abstract (HTML) (1377 Views)
Full-Text: (865 Views)
Introduction
Infertility is defined as the inability to achieve pregnancy after one year or more of unprotected intercourse [1]. Globally, the prevalence of infertility is about 9%. According to study in Iran, in 2020, the infertility rate was 13.2% and the prevalence of primary infertility rate was 17.3%, both are above the global average [2]. The World Health Organization (WHO) recognizes infertility as a significant reproductive health issue [3, 4]. The incidence of infertility increases with aging, such that the prevalence of primary infertility is 7.3-9.1% in married women aged 15-34, 25% in women aged 35-39, and 30% in women aged 40-44 [3, 5]. The prevalence of female infertility in developed countries is 37% [6]. The potential fertility can affect women’s social status, dignity, self-confidence, sense of adequacy, and worthiness, while the social pressures of infertility can lead to psychological issues such as sadness, depression, and distress [7, 8]. Psychological problems are related to the nature of infertility, ineffective medical interventions, high treatment costs, and unpredictable outcomes [9]. Although both men and women are emotionally affected by infertility, women suffer from more pressure than men [10, 11]. Infertility can cause huge amount of stress and emotional distress in women [12]. Distress occurs when stress is severe, prolonged, or both. Severe emotional distress is often associated with the diagnosis of infertility. Various definitions exist for distress, but it is commonly defined as a negative emotional state where the individual’s adaptive and coping processes fail to restore physiological and psychological balance [13]. Although the cause-and-effect relationship between distress and infertility is not clear, infertility is definitely linked to high distress [12-15].
Currently, the use of psychological interventions for infertile people is increasing [16-20]. The interventions include cognitive-behavioral therapy, mindfulness-based intervention (MBI), mind-body interventions, acceptance and commitment therapy, herbal therapy, internet-based interventions, and emotion/problem-oriented interventions [16-20]. In a recent study, the MBI was shown to successfully improve the mental health of women undergoing their first in-vitro fertilization (IVF) [21]. The clinical efficacy MBI has also been reported. This psychotherapy method is widely used for treating those experiencing distress in various medical and psychiatric conditions [22-25]. Recent studies have shown that MBI can break the vicious cycle of negative thoughts associated with infertility [22-25]. However, a study showed the ineffectiveness of a social-psychological intervention in altering mental health and pregnancy rates [20]. Systematic reviews have shown that the effectiveness of MBI in couples or individuals with infertility is greater than that of other psychological treatments in reducing psychological symptoms, stress, and anxiety [23]. Evidence suggests that MBIs are more effective than traditional cognitive therapy, behavioral therapy, or cognitive-behavioral therapy in treating infertility, because they address a broader range of problems, including interpersonal, marital, social, occupational, and psychological problems [26-31].
Patients undergoing infertility treatments often find the related information on the Internet [32-34]. A systematic review of 19 studies by Zillien et al. showed that the main reasons for the use of the Internet by infertile couples are the availability of a large amount of diverse information and the provision of emotional, social, and psychological support, which can lead to perceived improvements in knowledge, emotional state, relationships, and self-efficacy. However, they have concerns about the quality of information and its potential negative effects [32]. Internet-based interventions are a promising new approach for infertile patients, which need further development and testing [35-39]. Most of these programs are less expensive and can be affordable for users [27]. To our knowledge, there is no clinical trial on the effect of internet-based MBI on the emotional distress of infertile women in Iran or other countries. Therefore, this study aims to examine the effect of an online MBI on the infertility-related distress and stress and quality of life (QoL)of infertile women under treatment.
Materials and Methods
Study design, sampling, and allocation
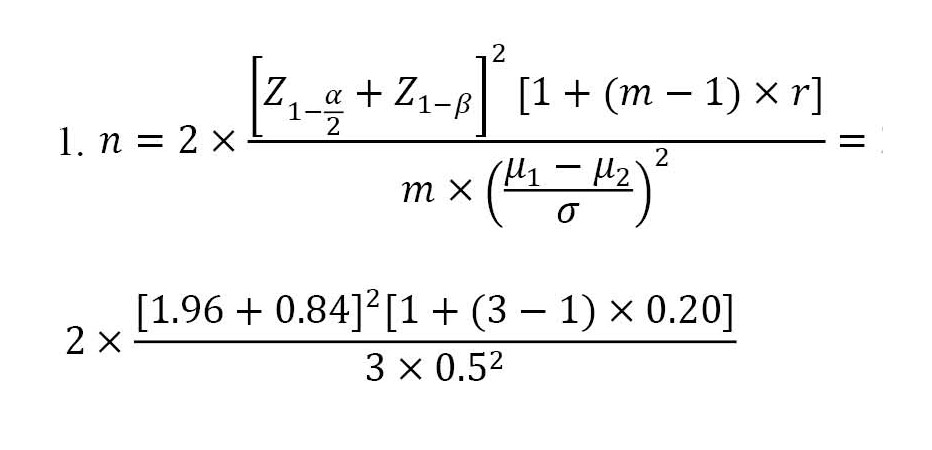
This is a protocol study outlining a double-blind randomized controlled clinical trial. Considering the main goal of this study, the sample size is determined 30 per group based on a previous study [39] and using the Equation 1, where the first type error (α)=0.05, second type error (β)=0.20, number of repetitions (m)=3, correlation coefficient between pre-test and post-test phases (r)=0.2, and effect size=0.5. To increase the study’s accuracy and considering the potential sample dropouts, the sample size will be determined as 35 per group (total=70).
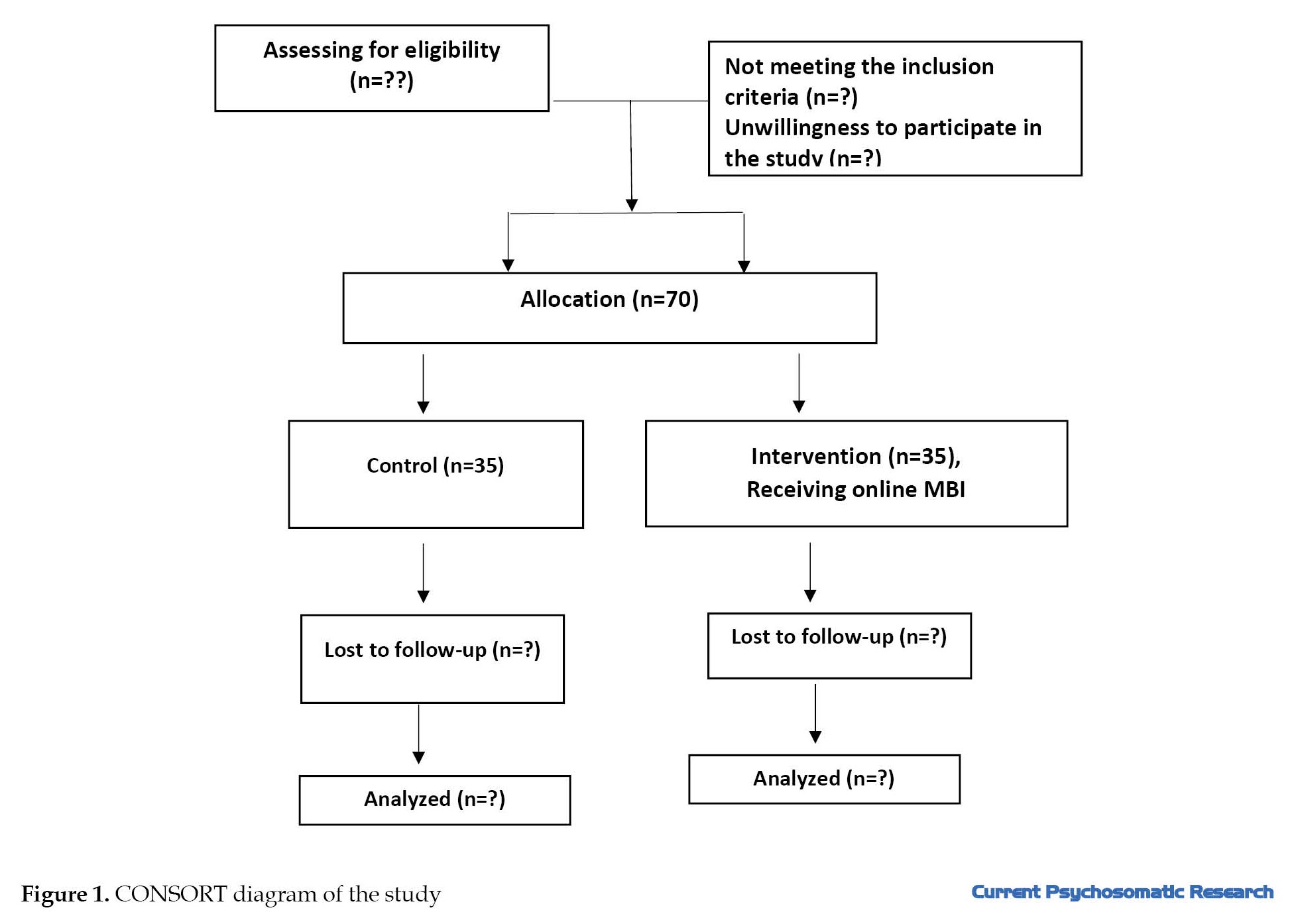
The participants will be selected based on inclusion criteria using a convenience sampling method from among infertile women undergoing infertility treatments referred to health centers, clinics, private offices, and infertility centers in Mazandaran Province, Iran. Inclusion criteria are: Iranian nationality, fluency in Persian, having a smartphone and being able to use them, age <45 years, diagnosed infertility, undergoing assisted reproductive techniques (IVF, IUI), and an anti-müllerian hormone level >1.5 ng/mL [40]. Exclusion criteria are: Intention to use donated embryos or eggs or surrogacy, canceling or terminating the treatment plan for any reason by the physician, receiving psychological or psychiatric counseling at the time of the study or in the past month, having major psychiatric disorders, having systemic diseases such as diabetes, hypertension, hyperlipidemia, and thyroid disorders (based on the medical records or self-report), experiencing the death of a relative or a major accident at least three months before the intervention, pregnancy detected by a blood test during the study, use of psychiatric medications (based on self-report), having an adopted child, smoking, smoking cigarette, hookah or alcohol consumption, history of previous marriage, and the need to receive prescribed psychotropic medications or psychotherapy counseling during the study. Using the block randomization method (14 blocks of five), participants will be assigned into two groups of intervention and control (Figure 1).
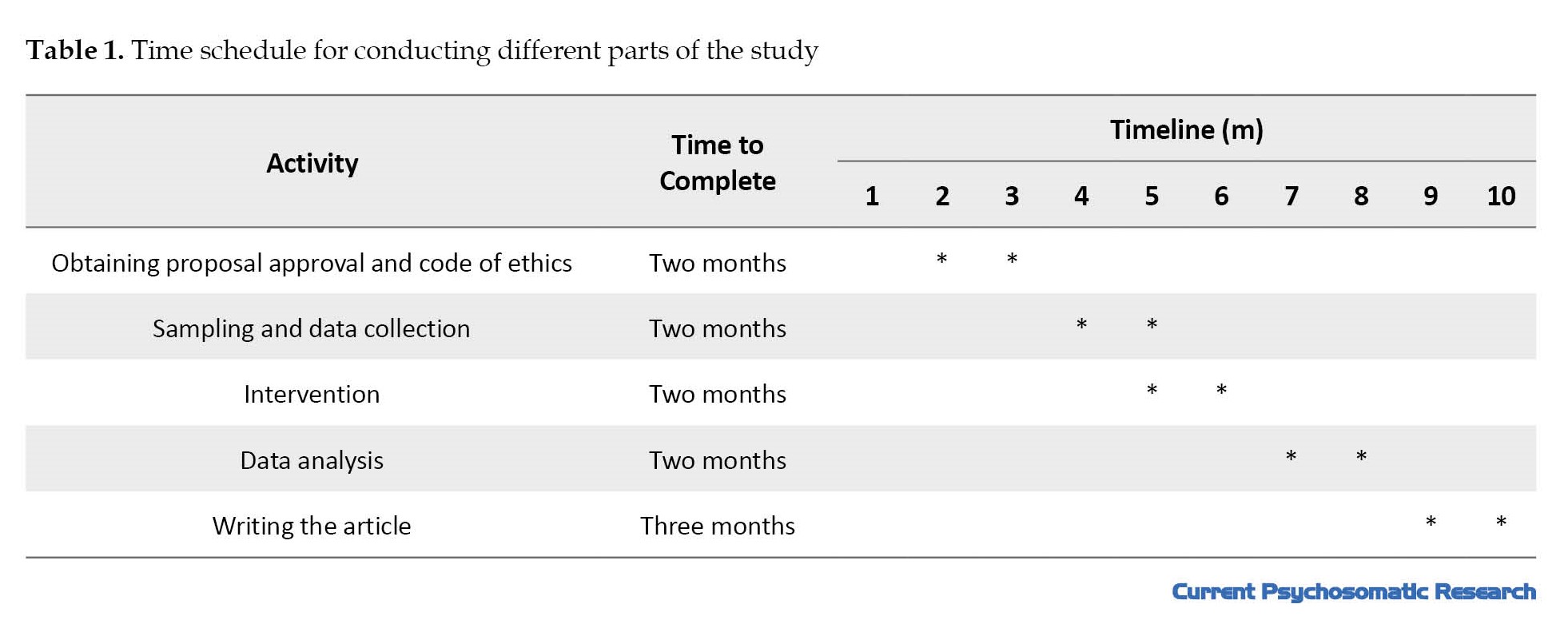
 In this study, due to the counseling and therapeutic nature, participants will be aware of the intervention. However, the data analyzer and the one conducted sampling will be unaware of allocation at the time of evaluation. The time schedule for conducting different parts of the study is provided in Table 1.
In this study, due to the counseling and therapeutic nature, participants will be aware of the intervention. However, the data analyzer and the one conducted sampling will be unaware of allocation at the time of evaluation. The time schedule for conducting different parts of the study is provided in Table 1.
Data collection tools
The data will be collected before the intervention, immediately after, and four weeks after the intervention from the two groups using five instruments:
The sociodemographic/medical-fertility form: This form surveys demographic and family related information (age, educational level, husband’s educational level, occupation, husband’s occupation, place of residence, duration of marriage, menstrual status, body mass index, and socio-economic status) as well as the information related to infertility and its treatment (infertility period, treatment period, and the cause of infertility);
General health questionnaire-28 (GHQ-28): This tool is a widely used screening tool designed by Goldberg in 1972 to identify mental disorders in medical settings and various situations. It has been translated into 38 languages and is utilized globally. The original version has 60 items, while its shorter forms have been developed with 12 and 28 items. The 28-item version has higher validity, sensitivity, and specificity compared to other versions [41]. The reported validity and reliability rates of 83% and 87%, respectively. For the Persian version, Taghavi assessed the test re-test reliability, split-half reliability, and internal consistency whose coefficients were 0.70, 0.93, and 0.90, respectively. The correlation coefficients between the subtests ranged from 0.72 to 0.87 [41].
Fertility problem inventory (FPI): This tool was developed by Newton et al. in 1999 to measure the infertility-related stress. It has 46 items and five domains: Social concern (10 items), sexual concern (8 items), relationship concern (10 items), rejection of childfree lifestyle (8 items), and need for parenthood (10 items). The items are rated on a 6-point scale ranging from 1 (completely disagree) to 6 (completely agree). The total score for the social concern, relationship concern, and need for parenthood domains range from 10 to 60, while for the sexual concern and rejection of childfree lifestyle domains, the total score ranges from 8 to 48. The score for the overall scale ranges from 46 to 276, with higher scores indicating greater infertility-related stress [42]. The validity and reliability of the Persian FPI were assessed in Iran by Alizadeh et al. in 2006 on 30 infertile individuals (15 men and 15 women) at Imam Khomeini Hospital. Cronbach’s α values were reported as 0.78 for social concern, 0.77 for sexual concern, 0.78 for relationship concern, 0.75 for rejection of childfree lifestyle, 0.84 for the need for parenthood, and 0.91 for the overall scale, confirming its reliability to be used in Iranian samples [43].
Infertility distress scale (IDS): The IDS is a 21-item tool designed by Akyuz et al. in Turkey in 2008 to assess distress among infertile individuals. It has a Cronbach’s α value of 0.933, indicating a high reliability [44]. For Iranian samples, the IDS’s validity and reliability were evaluated in 2010 by Arab Sheybani et al. on 300 women, including 145 fertile and 155 infertile. Their study confirmed that all 21 items correlated significantly with the overall scale, and the Cronbach’s α for the overall scale was 0.91. Its subscales could explain 88% of the total variance with an eigenvalue greater than 1, demonstrating its adequacy for measuring infertility distress in Iranian women [45].
QoL scale for infertile women: This is a 25-item tool designed by Kiani et al. in 2020. It has seven subscales: Psychological effects, sexual life, family and social effects, related concerns, physical effects, adaptive approaches, and inhibitory factors preventing adaptation. The tool has acceptable validity and reliability. Its concurrent validity is 0.61, with the intraclass correlation coefficient of 0.97, and a Cronbach’s α value of 0.87 [46].
Visual analog scale for satisfaction with intervention: The visual analog scale will be used in this study to measure participants’ satisfaction with the counseling sessions. It asks respondents to rate their level of satisfaction on a scale from 0 (not satisfied at all) to 10 (very satisfied). Scores are categorized as follows: 1-3 for low satisfaction, 4-7 for moderate satisfaction, and 8-10 for high satisfaction [47].
Intervention
The intervention group will receive online MBI at four sessions on Skyroom platform, after inviting them using the link sent on social network such as WhatsApp. The session 1 includes mindful breathing and body scan mediation; session 2: Guided imagery, kindness, and compassion; session 3: Mindful eating and mindful movements such as walking; session 4: Mindful conversations and observation of emotions. Women in the control group will receive routine care from their treatment centers or private physicians. After the end of the study, one MBI session will be provided to the control group.
Data analysis
Data will be analyzed in SPSS software, version 25. Normality will be assessed using the Shapiro-Wilk test. Descriptive statistics (Mean±SD, median, and percentages) will be used for describing the data. Inferential statistics will be parametric tests such as t-test, ANOVA (for comparing means), and Pearson’s correlation test for quantitative data. Non-parametric tests such as Mann-Whitney U test, Kruskal Wallis test, and Spearman’s correlation test will be used if the normality was rejected. Repeated measures ANOVA or ANCOVA will assess changes in scores over time. The intention-to-treat analysis will be used if the participants left during the study. Multiple linear regression and general linear models will assess the effect of sociodemographic factors on the dependent variables. The significance level for all tests will be set at 0.05.
Discussion
The primary goal of this study is to use MBI for improving the mental health of infertile women in Iran. Infertility can lead to various psychological responses in couples, such as reduced self-esteem, anger, sadness, difficulties planning for the future, social isolation, feelings of emptiness, jealousy of other couples with children, anxiety, and depression.
Mindfulness refers to deliberate, non-judgmental attention to thoughts, emotions, and sensations in the present moment. Since the emotional distress caused by infertility significantly affects treatment processes and all aspects of life, especially in infertile women, this study will use online method to provide better accessibility and effectiveness for the participants and, if successful, introduce a new psychological method to the therapists to help them focus on or address emotional distress, when necessary. This protocol-based study may help alleviate the emotional distress of infertile women and thus improve their mental health.
Limitations
The use of virtual networks for recruitment or intervention may avoid the women with a lack access to the Internet or smartphones from participating in this research. Additionally, data collection will be done using self-report tools.
Strengths
This protocol has a registered IRCT code. The use of online method will eliminate the need for commuting and will reduce costs for participants. Another strength is the blinding of the rater. The session contents will be developed based on a protocol assessed by experts that are not a member of the research team.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles will be considered in this study. Ethical approval has been obtained from the Ethics Committee of Mazandaran University of Medical Sciences (Code: MAZUMS.REC.332) and was registered by Iranian Registry of Clinical Trials (IRCT) (Code: IRCT20160619028528N7).
Funding
This project was funded by the Student Research Committee of Mazandaran University of Medical Sciences.
Authors' contributions
Investigation: Negin Salarian and Zeinab Hamzeh Gardeshi; Data collection: Forouzan Eliasi and Negin Salarian; Writing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Student Research Committee of Mazandaran University of Medical Sciences for their financial support.
References
Infertility is defined as the inability to achieve pregnancy after one year or more of unprotected intercourse [1]. Globally, the prevalence of infertility is about 9%. According to study in Iran, in 2020, the infertility rate was 13.2% and the prevalence of primary infertility rate was 17.3%, both are above the global average [2]. The World Health Organization (WHO) recognizes infertility as a significant reproductive health issue [3, 4]. The incidence of infertility increases with aging, such that the prevalence of primary infertility is 7.3-9.1% in married women aged 15-34, 25% in women aged 35-39, and 30% in women aged 40-44 [3, 5]. The prevalence of female infertility in developed countries is 37% [6]. The potential fertility can affect women’s social status, dignity, self-confidence, sense of adequacy, and worthiness, while the social pressures of infertility can lead to psychological issues such as sadness, depression, and distress [7, 8]. Psychological problems are related to the nature of infertility, ineffective medical interventions, high treatment costs, and unpredictable outcomes [9]. Although both men and women are emotionally affected by infertility, women suffer from more pressure than men [10, 11]. Infertility can cause huge amount of stress and emotional distress in women [12]. Distress occurs when stress is severe, prolonged, or both. Severe emotional distress is often associated with the diagnosis of infertility. Various definitions exist for distress, but it is commonly defined as a negative emotional state where the individual’s adaptive and coping processes fail to restore physiological and psychological balance [13]. Although the cause-and-effect relationship between distress and infertility is not clear, infertility is definitely linked to high distress [12-15].
Currently, the use of psychological interventions for infertile people is increasing [16-20]. The interventions include cognitive-behavioral therapy, mindfulness-based intervention (MBI), mind-body interventions, acceptance and commitment therapy, herbal therapy, internet-based interventions, and emotion/problem-oriented interventions [16-20]. In a recent study, the MBI was shown to successfully improve the mental health of women undergoing their first in-vitro fertilization (IVF) [21]. The clinical efficacy MBI has also been reported. This psychotherapy method is widely used for treating those experiencing distress in various medical and psychiatric conditions [22-25]. Recent studies have shown that MBI can break the vicious cycle of negative thoughts associated with infertility [22-25]. However, a study showed the ineffectiveness of a social-psychological intervention in altering mental health and pregnancy rates [20]. Systematic reviews have shown that the effectiveness of MBI in couples or individuals with infertility is greater than that of other psychological treatments in reducing psychological symptoms, stress, and anxiety [23]. Evidence suggests that MBIs are more effective than traditional cognitive therapy, behavioral therapy, or cognitive-behavioral therapy in treating infertility, because they address a broader range of problems, including interpersonal, marital, social, occupational, and psychological problems [26-31].
Patients undergoing infertility treatments often find the related information on the Internet [32-34]. A systematic review of 19 studies by Zillien et al. showed that the main reasons for the use of the Internet by infertile couples are the availability of a large amount of diverse information and the provision of emotional, social, and psychological support, which can lead to perceived improvements in knowledge, emotional state, relationships, and self-efficacy. However, they have concerns about the quality of information and its potential negative effects [32]. Internet-based interventions are a promising new approach for infertile patients, which need further development and testing [35-39]. Most of these programs are less expensive and can be affordable for users [27]. To our knowledge, there is no clinical trial on the effect of internet-based MBI on the emotional distress of infertile women in Iran or other countries. Therefore, this study aims to examine the effect of an online MBI on the infertility-related distress and stress and quality of life (QoL)of infertile women under treatment.
Materials and Methods
Study design, sampling, and allocation
This is a protocol study outlining a double-blind randomized controlled clinical trial. Considering the main goal of this study, the sample size is determined 30 per group based on a previous study [39] and using the Equation 1, where the first type error (α)=0.05, second type error (β)=0.20, number of repetitions (m)=3, correlation coefficient between pre-test and post-test phases (r)=0.2, and effect size=0.5. To increase the study’s accuracy and considering the potential sample dropouts, the sample size will be determined as 35 per group (total=70).
The participants will be selected based on inclusion criteria using a convenience sampling method from among infertile women undergoing infertility treatments referred to health centers, clinics, private offices, and infertility centers in Mazandaran Province, Iran. Inclusion criteria are: Iranian nationality, fluency in Persian, having a smartphone and being able to use them, age <45 years, diagnosed infertility, undergoing assisted reproductive techniques (IVF, IUI), and an anti-müllerian hormone level >1.5 ng/mL [40]. Exclusion criteria are: Intention to use donated embryos or eggs or surrogacy, canceling or terminating the treatment plan for any reason by the physician, receiving psychological or psychiatric counseling at the time of the study or in the past month, having major psychiatric disorders, having systemic diseases such as diabetes, hypertension, hyperlipidemia, and thyroid disorders (based on the medical records or self-report), experiencing the death of a relative or a major accident at least three months before the intervention, pregnancy detected by a blood test during the study, use of psychiatric medications (based on self-report), having an adopted child, smoking, smoking cigarette, hookah or alcohol consumption, history of previous marriage, and the need to receive prescribed psychotropic medications or psychotherapy counseling during the study. Using the block randomization method (14 blocks of five), participants will be assigned into two groups of intervention and control (Figure 1).
Data collection tools
The data will be collected before the intervention, immediately after, and four weeks after the intervention from the two groups using five instruments:
The sociodemographic/medical-fertility form: This form surveys demographic and family related information (age, educational level, husband’s educational level, occupation, husband’s occupation, place of residence, duration of marriage, menstrual status, body mass index, and socio-economic status) as well as the information related to infertility and its treatment (infertility period, treatment period, and the cause of infertility);
General health questionnaire-28 (GHQ-28): This tool is a widely used screening tool designed by Goldberg in 1972 to identify mental disorders in medical settings and various situations. It has been translated into 38 languages and is utilized globally. The original version has 60 items, while its shorter forms have been developed with 12 and 28 items. The 28-item version has higher validity, sensitivity, and specificity compared to other versions [41]. The reported validity and reliability rates of 83% and 87%, respectively. For the Persian version, Taghavi assessed the test re-test reliability, split-half reliability, and internal consistency whose coefficients were 0.70, 0.93, and 0.90, respectively. The correlation coefficients between the subtests ranged from 0.72 to 0.87 [41].
Fertility problem inventory (FPI): This tool was developed by Newton et al. in 1999 to measure the infertility-related stress. It has 46 items and five domains: Social concern (10 items), sexual concern (8 items), relationship concern (10 items), rejection of childfree lifestyle (8 items), and need for parenthood (10 items). The items are rated on a 6-point scale ranging from 1 (completely disagree) to 6 (completely agree). The total score for the social concern, relationship concern, and need for parenthood domains range from 10 to 60, while for the sexual concern and rejection of childfree lifestyle domains, the total score ranges from 8 to 48. The score for the overall scale ranges from 46 to 276, with higher scores indicating greater infertility-related stress [42]. The validity and reliability of the Persian FPI were assessed in Iran by Alizadeh et al. in 2006 on 30 infertile individuals (15 men and 15 women) at Imam Khomeini Hospital. Cronbach’s α values were reported as 0.78 for social concern, 0.77 for sexual concern, 0.78 for relationship concern, 0.75 for rejection of childfree lifestyle, 0.84 for the need for parenthood, and 0.91 for the overall scale, confirming its reliability to be used in Iranian samples [43].
Infertility distress scale (IDS): The IDS is a 21-item tool designed by Akyuz et al. in Turkey in 2008 to assess distress among infertile individuals. It has a Cronbach’s α value of 0.933, indicating a high reliability [44]. For Iranian samples, the IDS’s validity and reliability were evaluated in 2010 by Arab Sheybani et al. on 300 women, including 145 fertile and 155 infertile. Their study confirmed that all 21 items correlated significantly with the overall scale, and the Cronbach’s α for the overall scale was 0.91. Its subscales could explain 88% of the total variance with an eigenvalue greater than 1, demonstrating its adequacy for measuring infertility distress in Iranian women [45].
QoL scale for infertile women: This is a 25-item tool designed by Kiani et al. in 2020. It has seven subscales: Psychological effects, sexual life, family and social effects, related concerns, physical effects, adaptive approaches, and inhibitory factors preventing adaptation. The tool has acceptable validity and reliability. Its concurrent validity is 0.61, with the intraclass correlation coefficient of 0.97, and a Cronbach’s α value of 0.87 [46].
Visual analog scale for satisfaction with intervention: The visual analog scale will be used in this study to measure participants’ satisfaction with the counseling sessions. It asks respondents to rate their level of satisfaction on a scale from 0 (not satisfied at all) to 10 (very satisfied). Scores are categorized as follows: 1-3 for low satisfaction, 4-7 for moderate satisfaction, and 8-10 for high satisfaction [47].
Intervention
The intervention group will receive online MBI at four sessions on Skyroom platform, after inviting them using the link sent on social network such as WhatsApp. The session 1 includes mindful breathing and body scan mediation; session 2: Guided imagery, kindness, and compassion; session 3: Mindful eating and mindful movements such as walking; session 4: Mindful conversations and observation of emotions. Women in the control group will receive routine care from their treatment centers or private physicians. After the end of the study, one MBI session will be provided to the control group.
Data analysis
Data will be analyzed in SPSS software, version 25. Normality will be assessed using the Shapiro-Wilk test. Descriptive statistics (Mean±SD, median, and percentages) will be used for describing the data. Inferential statistics will be parametric tests such as t-test, ANOVA (for comparing means), and Pearson’s correlation test for quantitative data. Non-parametric tests such as Mann-Whitney U test, Kruskal Wallis test, and Spearman’s correlation test will be used if the normality was rejected. Repeated measures ANOVA or ANCOVA will assess changes in scores over time. The intention-to-treat analysis will be used if the participants left during the study. Multiple linear regression and general linear models will assess the effect of sociodemographic factors on the dependent variables. The significance level for all tests will be set at 0.05.
Discussion
The primary goal of this study is to use MBI for improving the mental health of infertile women in Iran. Infertility can lead to various psychological responses in couples, such as reduced self-esteem, anger, sadness, difficulties planning for the future, social isolation, feelings of emptiness, jealousy of other couples with children, anxiety, and depression.
Mindfulness refers to deliberate, non-judgmental attention to thoughts, emotions, and sensations in the present moment. Since the emotional distress caused by infertility significantly affects treatment processes and all aspects of life, especially in infertile women, this study will use online method to provide better accessibility and effectiveness for the participants and, if successful, introduce a new psychological method to the therapists to help them focus on or address emotional distress, when necessary. This protocol-based study may help alleviate the emotional distress of infertile women and thus improve their mental health.
Limitations
The use of virtual networks for recruitment or intervention may avoid the women with a lack access to the Internet or smartphones from participating in this research. Additionally, data collection will be done using self-report tools.
Strengths
This protocol has a registered IRCT code. The use of online method will eliminate the need for commuting and will reduce costs for participants. Another strength is the blinding of the rater. The session contents will be developed based on a protocol assessed by experts that are not a member of the research team.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles will be considered in this study. Ethical approval has been obtained from the Ethics Committee of Mazandaran University of Medical Sciences (Code: MAZUMS.REC.332) and was registered by Iranian Registry of Clinical Trials (IRCT) (Code: IRCT20160619028528N7).
Funding
This project was funded by the Student Research Committee of Mazandaran University of Medical Sciences.
Authors' contributions
Investigation: Negin Salarian and Zeinab Hamzeh Gardeshi; Data collection: Forouzan Eliasi and Negin Salarian; Writing and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Student Research Committee of Mazandaran University of Medical Sciences for their financial support.
References
- No author. Infertility| reproductive health| CDC [Internet]. 2022. [Updated 2024 May 15]. Available from: [Link]
- Zarif Golbar Yazdi H, Aghamohammadian Sharbaf H, Kareshki H, Amirian M. Infertility and psychological and social health of Iranian infertile women: A systematic review. Iran J Psychiatry. 2020; 15(1):67-79. [DOI: 10.18502/ijps.v15i1.2441]
- Saei Ghare Naz M, Ozgoli G, Sayehmiri K. Prevalence of infertility in Iran: A systematic review and meta-analysis. Urol J. 2020; 17(4):338-45. [PMID]
- Insogna IG, Ginsburg ES. Infertility, inequality, and how lack of insurance coverage compromises reproductive autonomy. AMA J Ethics. 2018; 20(12):E1152-9. [DOI:10.1001/amajethics.2018.1152] [PMID]
- Riahi ME, Zarezade Mehrizi E. [A study on the gender differences in psycho-social consequences of infertility: Infertile couples using Yazd’ Infertility Center services (Persian)]. Women’s strategy Stud. 2012; 14(56):153-210. [Link]
- Valiani M, Abediyan S, Ahmadi SM, Pahlavanzadeh S, Hassanzadeh A. The effect of relaxation techniques to ease the stress in infertile women. Iran J Nurs Midwifery Res. 2010; 15(4):259-64. [PMID]
- Amini L, Ghorbani B, Afshar B. [The comparison of infertility stress and perceived social support in infertile women and spouses of infertile men (Persian)]. Iran J Nurs. 2020; 32(122):80-90. [DOI:10.29252/ijn.32.122.80]
- Stellar C, Garcia-Moreno C, Temmerman M, Van Der Poel S. A systematic review and narrative report of the relationship between infertility, subfertility, and intimate partner violence. Int J Gynecol Obstet. 2016; 133(1):3-8. [DOI:10.1016/j.ijgo.2015.08.012] [PMID]
- Wiweko B, Anggraheni U, Elvira SD, Lubis HP. Distribution of stress level among infertility patients. Middle East Fertil Soc J. 2017; 22(2):145-8. [DOI:10.1016/j.mefs.2017.01.005]
- Karaca A, Unsal G. Psychosocial problems and coping strategies among turkish women with infertility.Asian Nurs Res (Korean Soc Nurs Sci). 2015; 9(3):243-50. [DOI:10.1016/j.anr.2015.04.007] [PMID]
- Tarabusi M, Volpe A, Facchinetti F. Psychological group support attenuates distress of waiting in couples scheduled for assisted reproduction. J Psychosom Obstet Gynecol. 2004; 25(3-4):273-9. [DOI:10.1080/01674820400017905] [PMID]
- Rooney KL, Domar AD. The relationship between stress and infertility. Dialogues Clin Neurosci. 2018; 20(1):41-7.[DOI:10.31887/DCNS.2018.20.1/klrooney] [PMID]
- Clifton J, Parent J, Seehuus M, Worrall G, Forehand R, Domar A. An internet-based mind/body intervention to mitigate distress in women experiencing infertility: A randomized pilot trial. Plos One. 202; 15(3):e0229379. [DOI:10.1371/journal.pone.0229379] [PMID]
- Chi HJ, Park IH, Sun HG, Kim JW, Lee KH. Psychological distress and fertility quality of life (FertiQoL) in infertile Korean women: The first validation study of Korean FertiQoL. Clin Exp Reprod Med. 2016; 43(3):174-80. [DOI:10.5653/cerm.2016.43.3.174] [PMID]
- Boivin J, Appleton TC, Baetens P, Baron J, Bitzer J, Corrigan E, et al. Guidelines for counselling in infertility: Outline version. Hum Reprod. 2001; 16(6):1301-4. [DOI:10.1093/humrep/16.6.1301] [PMID]
- Gameiro S, Boivin J, Dancet E, de Klerk C, Emery M, Lewis-Jones C, et al. ESHRE guideline: Routine psychosocial care in infertility and medically assisted reproduction - A guide for fertility staff. Hum Reprod. 2015; 30(11):2476-85. [DOI:10.1093/humrep/dev177] [PMID]
- Bai CF, Cui NX, Xu X, Mi GL, Sun JW, Shao D, et al. Effectiveness of two guided self-administered interventions for psychological distress among women with infertility: A three-armed, randomized controlled trial. Hum Reprod. 2019; 34(7):1235-48. [DOI:10.1093/humrep/dez066] [PMID]
- Chu K, Zhang Q, Han H, Xu C, Pang W, Ma Y, et al. A systematic review and meta-analysis of nonpharmacological adjuvant interventionds for patients undergoing assisted reproductive technology treatment. Int J Gynecol Obstet. 2017; 139(3):268-77. [DOI:10.1002/ijgo.12310] [PMID]
- de Liz TM, Strauss B. Differential efficacy of group and individual/couple psychotherapy with infertile patients. Hum Reprod. 2005; 20(5):1324-32. [DOI:10.1093/humrep/deh743] [PMID]
- Ying L, Wu LH, Loke AY. The effects of psychosocial interventions on the mental health, pregnancy rates, and marital function of infertile couples undergoing in vitro fertilization: A systematic review. J Assist Reprod Genet. 2016; 33(6):689-701. [PMID]
- Saunders PA, Tractenberg RE, Chaterji R, Amri H, Harazduk N, Gordon J, et al. Promoting self-awareness and reflection through an experiential mind-body skills course for first year medical students. Med Teach. 2007; 29(8):778-84. [DOI:10.1080/01421590701509647] [PMID]
- Patel A, Sharma PSVN, Kumar P. Application of mindfulness-based psychological interventions in infertility. J Hum Reprod Sci. 2020; 13(1):3-21. [DOI:10.4103/jhrs.JHRS_51_19] [PMID]
- Katyal N, Poulsen CM, Knudsen UB, Frederiksen Y. The association between psychosocial interventions and fertility treatment outcome: A systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2021; 259:125-32. [DOI:10.1016/j.ejogrb.2021.02.012] [PMID]
- Fard TR, Kalantarkousheh M, Faramarzi M. Effect of mindfulness-based cognitive infertility stress therapy on psychological well-being of women with infertility. Middle East Fertil Soc J. 2018; 23(4):476-81. [DOI:10.1016/j.mefs.2018.06.001]
- Galhardo A, Cunha M, Pinto-Gouveia J. Mindfulness-Based Program for Infertility: Efficacy study. Fertil Steril. 2013; 100(4):1059-67. [DOI:10.1016/j.fertnstert.2013.05.036] [PMID]
- Hamzehgardeshi Z, Yazdani F, Elyasi F, Moosazadeh M, Peyvandi S, Samadaee Gelehkolaee K, et al. The efficacy of group counselling on perceived stress among infertile women undergoing in vitro fertilization treatment: An RCT. Int J Reprod Biomed. 2019; 17(1):57-66. [DOI:10.18502/ijrm.v17i1.3821] [PMID]
- Sexton MB, Byrd MR, O’Donohue WT, Jacobs NN. Web-based treatment for infertility-related psychological distress. Arch Womens Ment Health. 2010; 13(4):347-58. [DOI:10.1007/s00737-009-0142-x] [PMID]
- Yazdani F, Elyasi F, Peyvandi S, Moosazadeh M, Galekolaee KS, Kalantari F, et al. Counseling-supportive interventions to decrease infertile women’s perceived stress: A systematic review. Electron Physician. 2017; 9(6):4694-702. [DOI:10.19082/4694] [PMID]
- Coffey KA, Hartman M. Mechanisms of action in the inverse relationship between mindfulness and psychological distress. Complement Health Pract Rev. 2008; 13(2):79-91. [DOI:10.1177/1533210108316307]
- Boivin J, Griffiths E, Venetis CA. Emotional distress in infertile women and failure of assisted reproductive technologies: meta-analysis of prospective psychosocial studies. BMJ. 2011; 342:d223. [PMID]
- Frederiksen Y, Farver-Vestergaard I, Skovgård NG, Ingerslev HJ, Zachariae R. Efficacy of psychosocial interventions for psychological and pregnancy outcomes in infertile women and men: A systematic review and meta-analysis. BMJ Open. 2015; 5(1):e006592. [DOI:10.1136/bmjopen-2014-006592] [PMID]
- Zillien N, Haake G, Fröhlich G, Bense T, Souren D. Internet use of fertility patients: A systemic review of the literature. J Reproduct Med and Endocrinol. 2011; 8(4):281-7. [Link]
- Brochu F, Robins S, Miner SA, Grunberg PH, Chan P, Lo K, et al. Searching the internet for infertility information: A survey of patient needs and preferences. J Med Internet Res. 2019; 21(12):e15132. [DOI:10.2196/15132] [PMID]
- Sormunen T, Karlgren K, Aanesen A, Fossum B, Westerbotn M. The role of social media for persons affected by infertility. BMC Women's Health. 2020; 20(1):112. [DOI:10.1186/s12905-020-00964-0] [PMID]
- Haemmerli K, Znoj H, Berger T. Internet-based support for infertile patients: A randomized controlled study. J Behav Med. 2010; 33(2):135-46. [DOI:10.1007/s10865-009-9243-2] [PMID]
- Nery SF, Paiva SPC, Vieira ÉL, Barbosa AB, Sant’Anna EM, Casalechi M, et al. Mindfulness-based program for stress reduction in infertile women: Randomized controlled trial. Stress Health. 2019; 35(1):49-58. [DOI:10.1002/smi.2839] [PMID]
- van Dongen AJ, Nelen WL, IntHout J, Kremer JA, Verhaak CM. e-Therapy to reduce emotional distress in women undergoing assisted reproductive technology (ART): A feasibility randomized controlled trial. Hum Reprod. 2016; 31(5):1046-57. [DOI:10.1093/humrep/dew040] [PMID]
- Domar AD, Rooney KL, Wiegand B, Orav EJ, Alper MM, Berger BM, et al. Impact of a group mind/body intervention on pregnancy rates in IVF patients. Fertil Steril. 2011; 95(7):2269-73. [DOI:10.1016/j.fertnstert.2011.03.046] [PMID]
- Elyasi F, Parkoohi PI, Naseri M, Gelekolaee KS, Hamedi M, Peyvandi S, et al. Relationship between coping/attachment styles and infertility-specific distress in Iranian infertile individuals: A cross-sectional study. Int J Reprod Biomed. 2021; 19(4):347-60. [PMID]
- Berek D, Novak E. Berek & Novak’s Gynecology. London: Wolters Kluwer Health - Ipsuk; 2019. [Link]
- Taghavi MR. [The normalization of general health questionnaire for Shiraz University Students (GHQ-28) (Persian)]. Daneshvar Raftar. 2008; 15(28):1-13. [Link]
- Newton CR, Sherrard W, Glavac I. The fertility problem inventory: Measuring perceived infertility-related stress. Fertil Steril. 1999; 72(1):54-62. [DOI:10.1016/S0015-0282(99)00164-8] [PMID]
- Alizadeh T, Farahani MN, Shahraray M, Alizadegan S. The relationship between self esteem and locus of control with infertility related stress of no related infertile men and women. J Reprod Infertil. 2005; 6(2):194-204. [Link]
- Akyuz A, Gürhan NE, Bakır B. [Development and validation of an infertility distress scale for Turkish women (Turkish)]. TAF Prev Med Bull. 2008; 7:469-76. [Link]
- Arab Sheybani K, Janbozorgi M, Akyuz A. Admissibility investigation and validation of infertility distress scale (IDS) in Iranian infertile women. Int J Fertil Steril. 2012; 6(1):37-44. [Link]
- Kiani Z, Simbar M, Hajian S, Zayeri F. Development and psychometric evaluation of a quality of life questionnaire for infertile women: A mixed method study. Reprod Health. 2020; 17(1):140. [DOI:10.1186/s12978-020-00988-7] [PMID]
- Tarhami F, Khadim S, Farajpour A, Baizaei H. [Validity and reliability examination of the Persian Version of the Iowa Satisfaction with Anesthesia Scale: The result of patient satisfaction with pain (Persian)]. Shefaye Khatam. 2018; 6(4):53-60 [DOI:10.29252/shefa.6.4.53]
Type of Study: Study protocol |
Subject:
Psychology
Received: 2023/12/11 | Accepted: 2024/03/2 | Published: 2023/10/1
Received: 2023/12/11 | Accepted: 2024/03/2 | Published: 2023/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
