Wed, May 27, 2026
[Archive]
Volume 2, Issue 2 (Winter 2024)
CPR 2024, 2(2): 87-96 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghanbari Jolfaei A, Rafiei M, Pirhayati M. Testing How Reliable and Accurate the Persian Version of the WHO Disability Assessment Schedule II is for People With Mental Health Issues. CPR 2024; 2 (2) :87-96
URL: http://cpr.mazums.ac.ir/article-1-70-en.html
URL: http://cpr.mazums.ac.ir/article-1-70-en.html



Department of Psychiatry, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 688 kb]
(519 Downloads)
| Abstract (HTML) (1100 Views)
Full-Text: (448 Views)
Introduction
Psychiatric disorders are among the significant causes of disability worldwide. The global burden of mental illness accounts for 32.4% of years lived with disability (YLDs) and 0.13% of disability-adjusted life years (DALYs). To reduce the personal, social and economic costs associated with mental illnesses, an accurate assessment of the extent of this disability is necessary [1]. To establish an accepted global framework for diagnosing and classifying disability, the World Health Organization (WHO) has developed an international classification for functioning, disability, and health [2], in which disability is defined as a problem at the body, personality, or social level in one or more areas of life [3]. Based on this definition, the WHO has created and presented the WHO disability assessment schedule II (WHODAS II) to evaluate disability according to the new definition [4], which introduces the measurement of functional decline resulting from diseases [5]. WHODAS II was designed in two versions, consisting of 12 and 36 items, which examine limitations across six dimensions: Understanding, self-care, mobility, interacting with other people, life activities and joining in community activities [5, 6]. Carlozzi et al. evaluated the reliability and validity of WHODAS II in patients with Huntington disease and demonstrated the reliability and validity of this questionnaire in them [7].
Andrew et al. assessed 8824 individuals across three groups, those with psychiatric illnesses, those with other diseases and healthy individuals, using WHODAS II. The results showed that psychiatric patients experienced more problems than healthy individuals and those with other diseases [8]. Ustün et al. examined the WHODAS II by interviewing 65000 people in two groups: The general population and individuals with specific diseases, using the 36- and 12-item versions of the WHODAS II. The results indicate that this questionnaire is a powerful tool for evaluating the abilities and disabilities of patients [5]. This questionnaire has been translated into different languages [5, 9] and utilized in research and clinical settings. However, no study demonstrated its reliability and validity for psychiatric patients in the Persian language. Given the use and importance of this tool, we decided to prepare its Persian version and evaluate it in terms of reliability and validity.
Materials and Methods
This psychometric study assessed the validity and reliability of the 12- and 36-item WHODAS II versions. A total of 129 hospitalized patients were selected through convenience sampling. The patients were admitted to the Psychiatry Department of Rasoul Akram and Iran Psychiatry University Hospitals, affiliated with the Iran University of Medical Sciences, between April 2017 and September 2017. Patients who did not wish to participate in the research or were in acute psychiatric conditions and unable to make accurate judgments about themselves and their surroundings were excluded from the study (inclusion criteria). Additionally, patients who did not provide the necessary information or completed the questionnaires were excluded from the study (exclusion criteria). Demographic information, including age, gender, marital status, and education level, was collected using a checklist.
All stages of preparation and evaluation of the questionnaire were conducted separately for the 12-item and 36-item versions. First, the WHODAS II was translated from English to Farsi by two psychiatrists who were fluent in English. Then, the two English versions were compared and united into a single Persian version. The Persian translation of the questionnaire was then translated back into English by another individual fluent in English who had not seen the original English text. After review and revision, the two English versions (direct and reverse) were merged into a single English version. Finally, the final version of the questionnaire was prepared in Persian. This translation was first provided to 9 Iran University of Medical Sciences faculty members for validation. After making final changes, it was administered to psychiatric patients hospitalized in two academic hospitals, Rasoul Akram and Iran Psychiatry.
Face validity was evaluated using a qualitative method based on faculty members’ opinions. The content validity was assessed based on the opinions of faculty members using a quantitative method by calculating the content validity ratio (CVR) and the content validity index (CVI). Simultaneously, while all patients completed the WHODAS II (both versions), half of the patients answered the EuroQol 5 dimension (EQ-5D) and short-form 36 (SF-36) questionnaires to compare the results with those of the WHODAS II. The reason for dividing the patients into two groups to fill out the standard questionnaires was to enhance patient acceptance and cooperation in this research. One week later, the WHODAS II was administered to those patients who had not been discharged from the hospital to determine the reliability of the test-re-test method.
SPSS software, version 23 was used for data analysis. To assess the validity of the questionnaire, the Pearson correlation coefficient was employed. The test-re-test method was utilized to evaluate the reliability and stability of the results. The Pearson correlation coefficient was calculated with a time interval of one week. To check the internal consistency, the Cronbach α was calculated.
Characteristics of the questionnaires
The demographic checklist contains demographic information of patients. SF-36 questionnaire examines 8 dimensions of quality of life and consists of 36 items. The dimensions include general health (5 items), physical function (10 items), mental health (5 items), social function (2 items), pain (2 items), physical role limitation (4 items), mental role limitation (3 items) and vitality (1 item). Additionally, an item measures health changes, which is not part of the 8 dimensions and is not scored. The items are scored based on the Likert scale, with scores for the 8 dimensions ranging from 0 to 100. This questionnaire has international reliability and validity, and in Iran, it has been translated, with its reliability and validity examined and confirmed by the academic center for education, culture and research [10].
EuroQol-5 questionnaire includes two descriptive sections and a visual scale. The first part consists of five dimensions: Mobility, self-care, daily activities, pain/discomfort and anxiety and depression, which together encompass 243 health states, along with two states of unconsciousness and death, completed by the patient’s caregivers. The visual scale is a 20 cm scale ranging from 0 (worst condition) to 100 (best condition), on which the individual marks their current health level. Test-re-test reliability has been reported to range from 0.69 to 0.94 for the original version and 0.86 for this version. The Kappa coefficient for test-re-test stability after seven days has been reported to range from 0.29 to 0.67, while Kendall’s correlation falls within the range of 0.25 to 0.64 [11]. In Iran, the reliability and validity of the Persian version were evaluated and confirmed [12].
Results
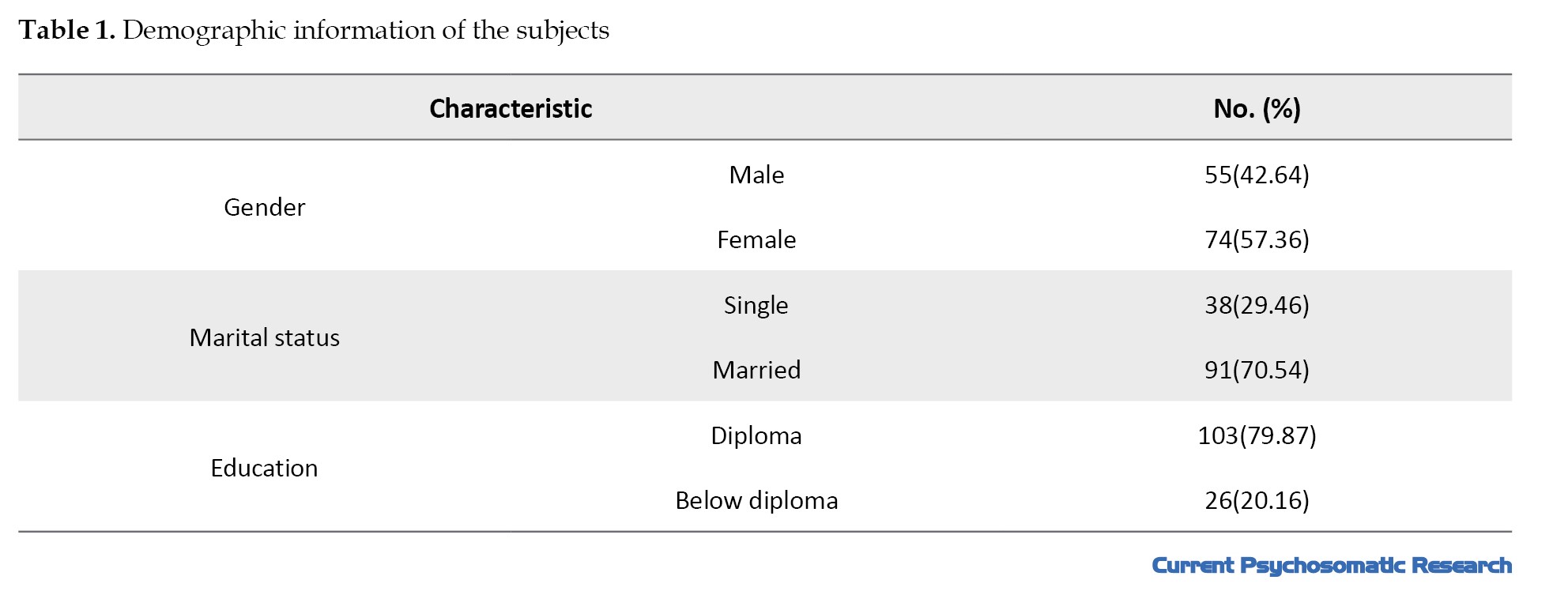
Of 129 patients who provided complete information through questionnaires and a demographic information checklist, 74(57.36%) were women and 55(42.64%) were men. The Mean±SD age of the subjects was 42.20±9.51 years (range: 29–62 years). Ninety-one individuals (70.54%) were married, while 38(29.46%) were single. Twenty-six individuals (20.16%) had a diploma, and 103(79.84%) had a diploma or higher (Table 1).
Face validity
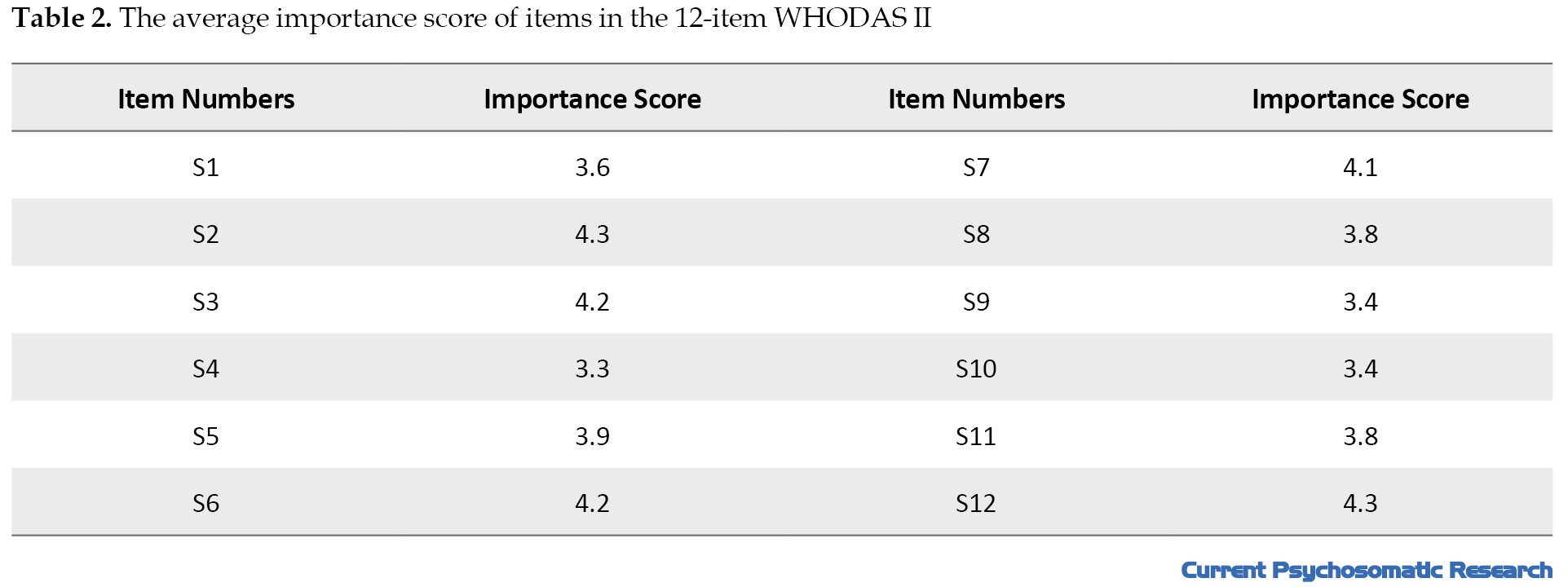
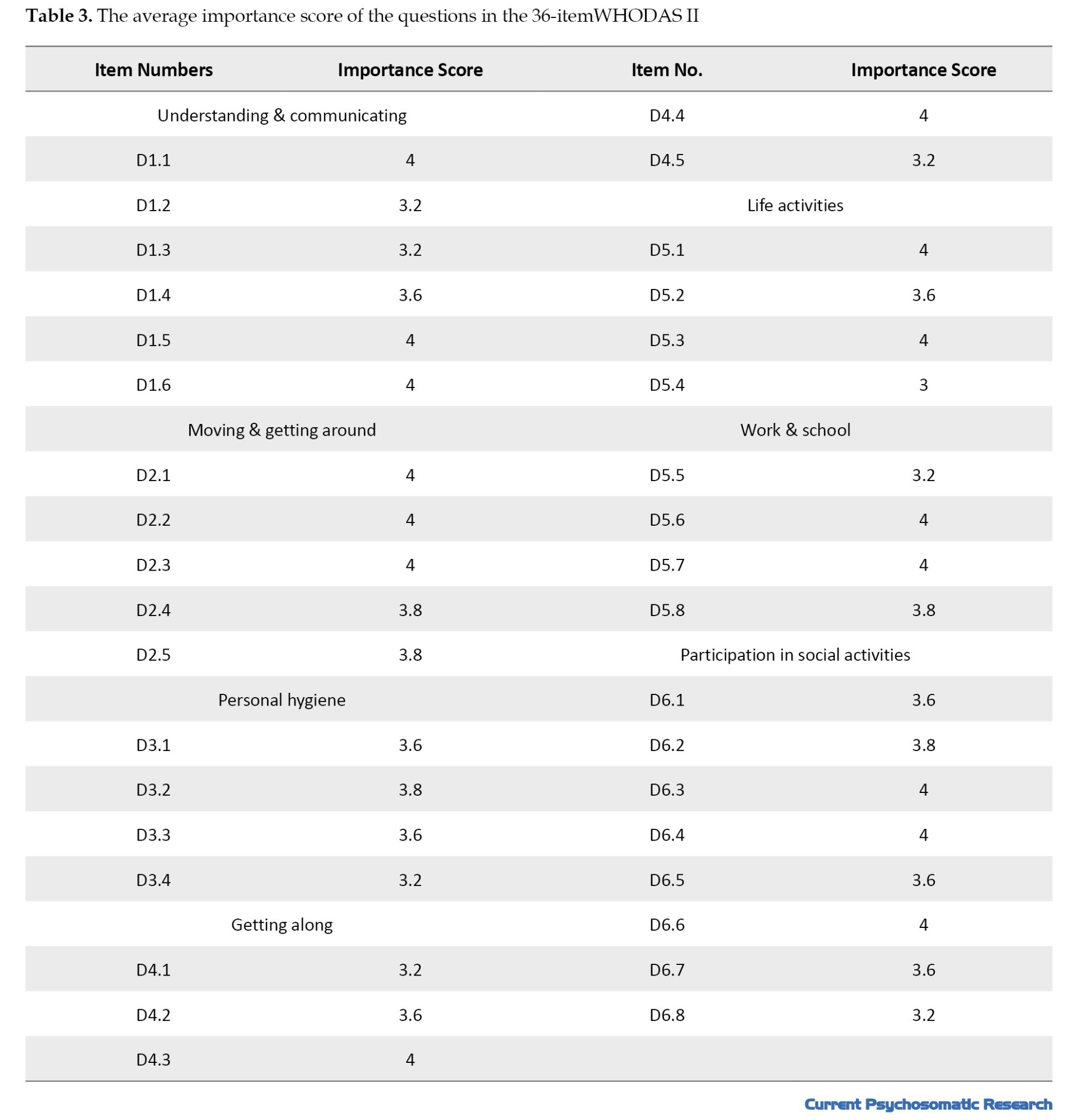
To qualitatively check the face validity, the 12-item and 36-item questionnaires were given to two faculty members fluent in English and familiar with specialized terms. They assessed the items using simple and understandable language while avoiding technical jargon, and their feedback was incorporated into the questionnaire [12]. Additionally, a pilot interview was conducted with five participants from the sample. Then, to quantitatively assess the face validity, 9 faculty members were asked to score each item of the two questionnaires (48 items in total) based on the importance of the questions. The significance of each item was calculated using the Equation 1:
1. Importance score=Σ(f×Importance)/n
Where f is the number of faculty members assigned an importance score (1 to 5) to each item and n is the total number of faculty members [12]. The importance scores for each item are presented in Tables 2 and 3.
Content validity
To qualitatively evaluate the content validity, 9 faculty members were interviewed to assess Persian grammar, the use of appropriate words, and the proper placement of items for each item. Their opinions were summarized and incorporated into the questionnaire. The evaluation of content validity was also conducted quantitatively based on the experts’ opinions by calculating the CVR and the CVI. The CVR was used to ensure that the most important and relevant content was selected for each item, while the CVI was used to verify the correct design of the items [12]. According to Lawshe, with the participation of 9 faculty members in this evaluation, the CVR for each item in the questionnaire must be greater than 0.78 to be considered valid [13-15]. In this study, the CVR for all questions of the 12-item and 36-item questionnaires was above 0.78, confirming the content validity of these questionnaires. Additionally, the CVI for all items of the 12-item- and 36-item questionnaire items ranged from 0.66 to 1.
Construct validity
Exploratory factor analysis was conducted for all the grouped items, and Bartlett’s test was significant, indicating a significant relationship between the items (P<0.001). The Kaiser–Meyer–Olkin (KMO) test was also performed to confirm sampling adequacy, yielding a KMO value 0.8, which is considered acceptable. These results demonstrated an internal correlation among the items.
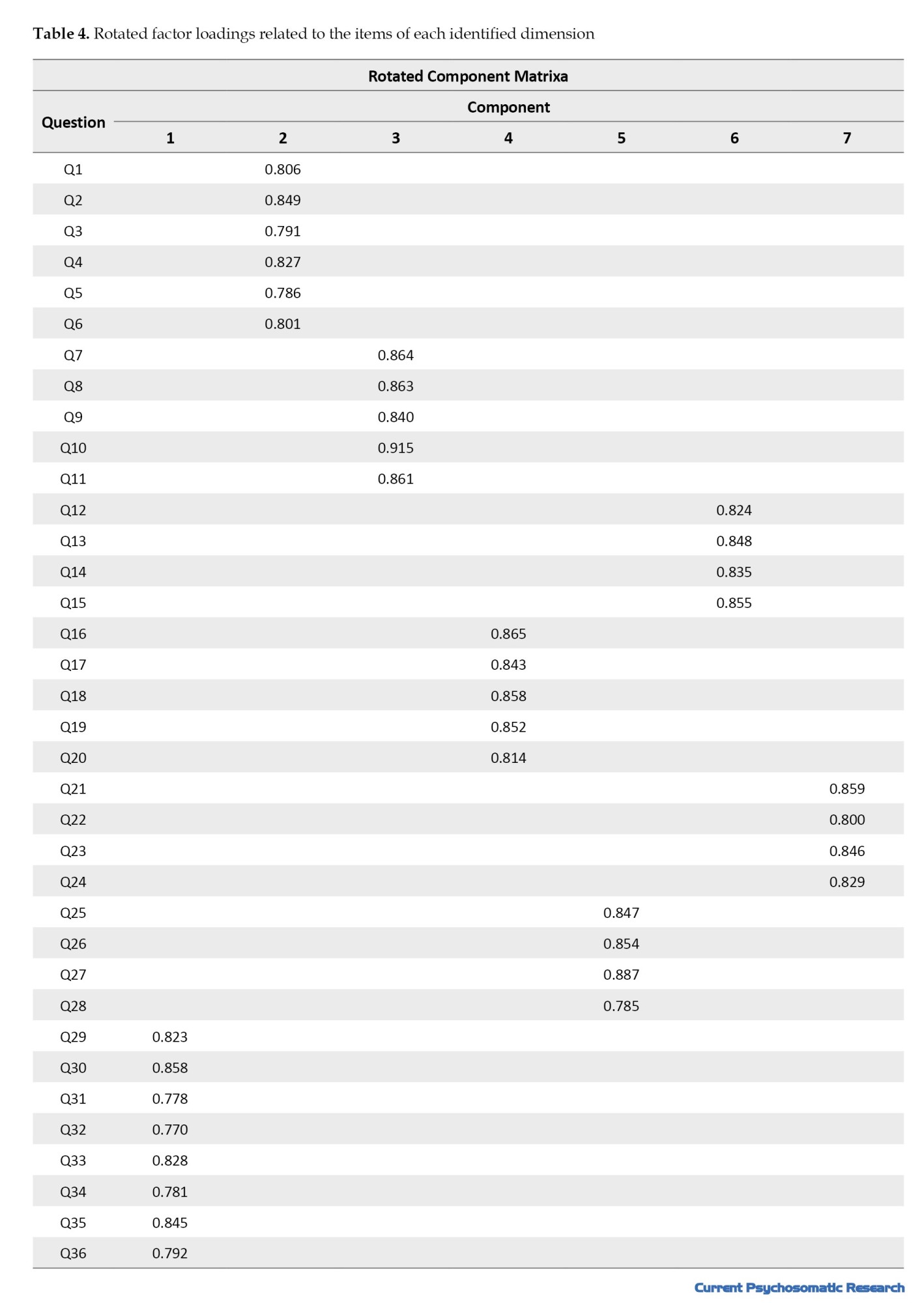
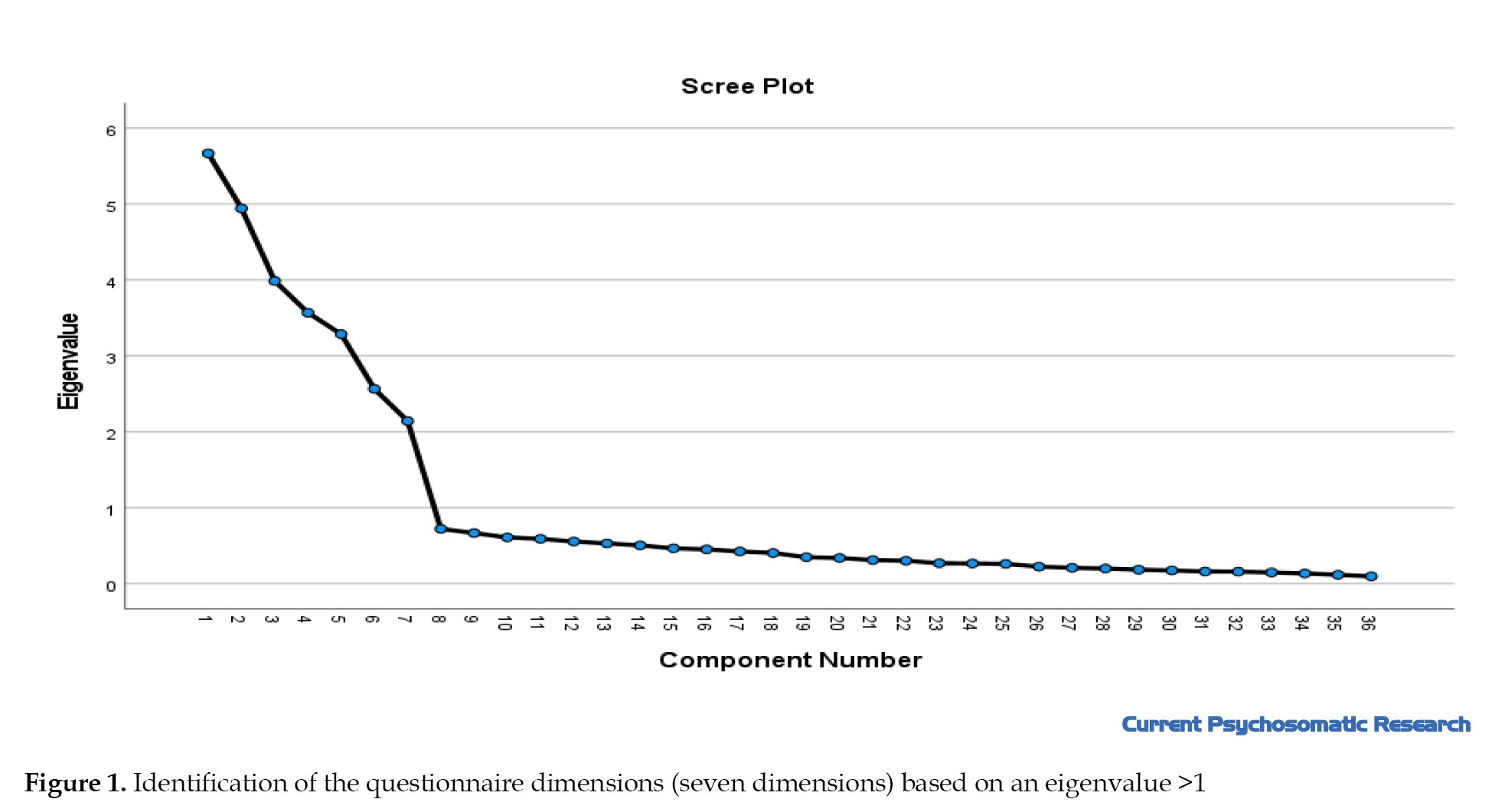
To carry out construct validity, the questionnaire items were divided into the specified dimensions, and the scores obtained from them were analyzed using the average variance extracted (AVE) and composite reliability (CR) tests. The factor loadings for all items were greater than 0.5, indicating that the items converged with the relevant factor. The scores obtained for each dimension in the AVE test were greater than 0.6 and the scores for the CR test were greater than 0.75. Accordingly, seven dimensions were identified with Varimax rotation, as illustrated in the scree plot diagram (Table 4 and Figure 1).
Reliability
A re-test was performed to determine the reliability or stability of the test results. The WHODAS II was completed one week later and the results were compared. The findings showed a correlation between the questionnaire scores from one week to the next. The intraclass correlation (ICC) value was 0.84 for the 12-item questionnaire and 0.81 for the 36-item questionnaire.
The Cronbach α was used to assess internal consistency, yielding values of 0.78 and 0.62 for the 12-item and 36-item questionnaires, respectively. Additionally, the Cronbach α values less than 0.6 were not improved by removing any of the items.
Discussion
The results of the present study indicated that the Persian version of the WHODAS II has acceptable validity and reliability for assessing disability. Overall, this questionnaire demonstrates good internal consistency and can be utilized in clinical research settings involving Persian-speaking psychiatric patients.
The Cronbach α coefficient for the 36-item questionnaire was 0.788, indicating that its Persian version has good internal consistency and removing any item does not reduce the Cronbach α value below 0.7. Conversely, overall, removing item D5.3, “Do you perform all tasks related to you in the family?” from the life activities dimension, and item D5.8, “Doing occupational-educational activities as soon as possible,” also from the life activities dimension, resulted in a greater increase in the Cronbach α value compared to the removal of other items. Regarding the item “Do you perform all tasks related to you in the family?” there is a possibility that the meaning of the item is not well understood by the respondent, as the phrase “related duties” may be interpreted differently by each individual. For some, the meaning of this phrase may not be entirely clear and asking such a question may lead to resistance to providing an accurate answer.
Regarding the item “carrying out occupational-educational activities as soon as possible,” the simultaneous mention of two fields, occupation, and education, in one sentence makes it difficult for respondents to distinguish between them. People’s interpretations of the item may vary. Additionally, individuals with different jobs and educational backgrounds will likely provide various responses to this item.
Borglin et al. assessed 162 cases with physical problems and 156 cases with mental issues from 15 centers, demonstrating an acceptable internal consistency with a Cronbach α of 0.77 and a test-re-test reliability ICC of 0.74, considered acceptable [16]. The results of our study showed that the Cronbach α value for the 36-item questionnaire was 0.788. Additionally, regarding test-re-test reliability, an ICC value of 0.81 was obtained, consistent with the study’s results mentioned above. Furthermore, in another study conducted in Greece involving 10163 patients, this questionnaire demonstrated acceptable internal consistency with the version prepared in Greek [17]. Carlozzi et al. evaluated the reliability and validity of WHODAS II, which were confirmed in patients with Huntington disease [7]. In another study in Singapore involving patients with psychiatric diagnoses, the validity and reliability of this questionnaire were also confirmed [18].
Garin et al. aimed to provide a structural explanation to measure the ability and disability of patients across Europe; 1119 patients with one of 17 chronic diseases in seven medical centers were evaluated using the WHODAS II. Additionally, the patients were followed up for 6 weeks and 3 months. They reported that the WHODAS II could accurately assess disability. To establish the validity of this questionnaire, the EQ-5D was used in this study [19].
The analysis of the reliability of the 12-item questionnaire showed that the obtained Cronbach α coefficient was 0.62, which was lower than that of the 36-item questionnaire. On the other hand, the general examination of the items indicates that removing items SI, “Standing for a long time like 30 minutes,” S5, “What effect did the problems have on your emotions and feelings?” S7, “Walking long distances like 1 km,” and S8, “Washing the whole body,” might result in higher Cronbach α values than the other items. Regarding item S5, “How did the problems affect your emotions and feelings?” it is possible that respondents may not fully understand the concept of influencing emotions and feelings, leading to varying answers from different individuals.
Concerning the 36-item questionnaire, the Cronbach α values for different dimensions were as follows: Understanding and communication: 0.76; mobility: 0.69; personal hygiene: 0.78; interacting with other people: 0.72; life activities: 0.75; and participation in social activities: 0.71. Additionally, for test-re-test reliability, the ICC value was found to be 0.81, with specific values of 0.88 for understanding and communication, 0.79 for mobility, 0.77 for personal hygiene, 0.69 for interacting with other people, 0.87 for life activities and 0.81 for participation in social activities.
Conclusion
These results indicate that the questionnaire items in Persian have better reliability in the dimensions of understanding and communication, life activities, and participation in social activities. The dimensions mentioned above exhibit less variability than other dimensions and are less susceptible to significant changes over time. One of the study’s limitations was its limited number of patients and the fact that it was only conducted at two university centers. Additionally, although efforts were made to provide the necessary training to participants before filling out the questionnaire and to request that it be completed in a calm environment with sufficient mental concentration, these considerations were not feasible in some cases. It is suggested that a study with a larger sample size be conducted in several centers, involving more participants in calm conditions and with more training before completing the questionnaire. It is recommended that the Persian version developed in this research be used for research and clinical purposes.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Iran University of Medical Sciences (IR.IUMS.FMD.REC 1396.9411286008). The data were also kept confidential.
Funding
The paper was extracted from the Medical Assistant Thesis of Masoume Rafiei, approved by Iran University of Medical Sciences and financially supported by Iran University of Medical Sciences.
Authors' contributions
Conceptualization and supervision: Atefeh Ghanbari; Research, writing the original draft, review and editing: Masoumeh Rafiei and Mohammad Pir Hayati; Data collection: Masoumeh Rafiei and Mohammad Pir Khaiti: Data analysis: Mohammad Pir Khaiti; Sources: all authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to all the officials of Rasool Akram Hospital and to everyone who assisted the researchers in any way during this study.
References
Psychiatric disorders are among the significant causes of disability worldwide. The global burden of mental illness accounts for 32.4% of years lived with disability (YLDs) and 0.13% of disability-adjusted life years (DALYs). To reduce the personal, social and economic costs associated with mental illnesses, an accurate assessment of the extent of this disability is necessary [1]. To establish an accepted global framework for diagnosing and classifying disability, the World Health Organization (WHO) has developed an international classification for functioning, disability, and health [2], in which disability is defined as a problem at the body, personality, or social level in one or more areas of life [3]. Based on this definition, the WHO has created and presented the WHO disability assessment schedule II (WHODAS II) to evaluate disability according to the new definition [4], which introduces the measurement of functional decline resulting from diseases [5]. WHODAS II was designed in two versions, consisting of 12 and 36 items, which examine limitations across six dimensions: Understanding, self-care, mobility, interacting with other people, life activities and joining in community activities [5, 6]. Carlozzi et al. evaluated the reliability and validity of WHODAS II in patients with Huntington disease and demonstrated the reliability and validity of this questionnaire in them [7].
Andrew et al. assessed 8824 individuals across three groups, those with psychiatric illnesses, those with other diseases and healthy individuals, using WHODAS II. The results showed that psychiatric patients experienced more problems than healthy individuals and those with other diseases [8]. Ustün et al. examined the WHODAS II by interviewing 65000 people in two groups: The general population and individuals with specific diseases, using the 36- and 12-item versions of the WHODAS II. The results indicate that this questionnaire is a powerful tool for evaluating the abilities and disabilities of patients [5]. This questionnaire has been translated into different languages [5, 9] and utilized in research and clinical settings. However, no study demonstrated its reliability and validity for psychiatric patients in the Persian language. Given the use and importance of this tool, we decided to prepare its Persian version and evaluate it in terms of reliability and validity.
Materials and Methods
This psychometric study assessed the validity and reliability of the 12- and 36-item WHODAS II versions. A total of 129 hospitalized patients were selected through convenience sampling. The patients were admitted to the Psychiatry Department of Rasoul Akram and Iran Psychiatry University Hospitals, affiliated with the Iran University of Medical Sciences, between April 2017 and September 2017. Patients who did not wish to participate in the research or were in acute psychiatric conditions and unable to make accurate judgments about themselves and their surroundings were excluded from the study (inclusion criteria). Additionally, patients who did not provide the necessary information or completed the questionnaires were excluded from the study (exclusion criteria). Demographic information, including age, gender, marital status, and education level, was collected using a checklist.
All stages of preparation and evaluation of the questionnaire were conducted separately for the 12-item and 36-item versions. First, the WHODAS II was translated from English to Farsi by two psychiatrists who were fluent in English. Then, the two English versions were compared and united into a single Persian version. The Persian translation of the questionnaire was then translated back into English by another individual fluent in English who had not seen the original English text. After review and revision, the two English versions (direct and reverse) were merged into a single English version. Finally, the final version of the questionnaire was prepared in Persian. This translation was first provided to 9 Iran University of Medical Sciences faculty members for validation. After making final changes, it was administered to psychiatric patients hospitalized in two academic hospitals, Rasoul Akram and Iran Psychiatry.
Face validity was evaluated using a qualitative method based on faculty members’ opinions. The content validity was assessed based on the opinions of faculty members using a quantitative method by calculating the content validity ratio (CVR) and the content validity index (CVI). Simultaneously, while all patients completed the WHODAS II (both versions), half of the patients answered the EuroQol 5 dimension (EQ-5D) and short-form 36 (SF-36) questionnaires to compare the results with those of the WHODAS II. The reason for dividing the patients into two groups to fill out the standard questionnaires was to enhance patient acceptance and cooperation in this research. One week later, the WHODAS II was administered to those patients who had not been discharged from the hospital to determine the reliability of the test-re-test method.
SPSS software, version 23 was used for data analysis. To assess the validity of the questionnaire, the Pearson correlation coefficient was employed. The test-re-test method was utilized to evaluate the reliability and stability of the results. The Pearson correlation coefficient was calculated with a time interval of one week. To check the internal consistency, the Cronbach α was calculated.
Characteristics of the questionnaires
The demographic checklist contains demographic information of patients. SF-36 questionnaire examines 8 dimensions of quality of life and consists of 36 items. The dimensions include general health (5 items), physical function (10 items), mental health (5 items), social function (2 items), pain (2 items), physical role limitation (4 items), mental role limitation (3 items) and vitality (1 item). Additionally, an item measures health changes, which is not part of the 8 dimensions and is not scored. The items are scored based on the Likert scale, with scores for the 8 dimensions ranging from 0 to 100. This questionnaire has international reliability and validity, and in Iran, it has been translated, with its reliability and validity examined and confirmed by the academic center for education, culture and research [10].
EuroQol-5 questionnaire includes two descriptive sections and a visual scale. The first part consists of five dimensions: Mobility, self-care, daily activities, pain/discomfort and anxiety and depression, which together encompass 243 health states, along with two states of unconsciousness and death, completed by the patient’s caregivers. The visual scale is a 20 cm scale ranging from 0 (worst condition) to 100 (best condition), on which the individual marks their current health level. Test-re-test reliability has been reported to range from 0.69 to 0.94 for the original version and 0.86 for this version. The Kappa coefficient for test-re-test stability after seven days has been reported to range from 0.29 to 0.67, while Kendall’s correlation falls within the range of 0.25 to 0.64 [11]. In Iran, the reliability and validity of the Persian version were evaluated and confirmed [12].
Results
Of 129 patients who provided complete information through questionnaires and a demographic information checklist, 74(57.36%) were women and 55(42.64%) were men. The Mean±SD age of the subjects was 42.20±9.51 years (range: 29–62 years). Ninety-one individuals (70.54%) were married, while 38(29.46%) were single. Twenty-six individuals (20.16%) had a diploma, and 103(79.84%) had a diploma or higher (Table 1).
Face validity
To qualitatively check the face validity, the 12-item and 36-item questionnaires were given to two faculty members fluent in English and familiar with specialized terms. They assessed the items using simple and understandable language while avoiding technical jargon, and their feedback was incorporated into the questionnaire [12]. Additionally, a pilot interview was conducted with five participants from the sample. Then, to quantitatively assess the face validity, 9 faculty members were asked to score each item of the two questionnaires (48 items in total) based on the importance of the questions. The significance of each item was calculated using the Equation 1:
1. Importance score=Σ(f×Importance)/n
Where f is the number of faculty members assigned an importance score (1 to 5) to each item and n is the total number of faculty members [12]. The importance scores for each item are presented in Tables 2 and 3.
Content validity
To qualitatively evaluate the content validity, 9 faculty members were interviewed to assess Persian grammar, the use of appropriate words, and the proper placement of items for each item. Their opinions were summarized and incorporated into the questionnaire. The evaluation of content validity was also conducted quantitatively based on the experts’ opinions by calculating the CVR and the CVI. The CVR was used to ensure that the most important and relevant content was selected for each item, while the CVI was used to verify the correct design of the items [12]. According to Lawshe, with the participation of 9 faculty members in this evaluation, the CVR for each item in the questionnaire must be greater than 0.78 to be considered valid [13-15]. In this study, the CVR for all questions of the 12-item and 36-item questionnaires was above 0.78, confirming the content validity of these questionnaires. Additionally, the CVI for all items of the 12-item- and 36-item questionnaire items ranged from 0.66 to 1.
Construct validity
Exploratory factor analysis was conducted for all the grouped items, and Bartlett’s test was significant, indicating a significant relationship between the items (P<0.001). The Kaiser–Meyer–Olkin (KMO) test was also performed to confirm sampling adequacy, yielding a KMO value 0.8, which is considered acceptable. These results demonstrated an internal correlation among the items.
To carry out construct validity, the questionnaire items were divided into the specified dimensions, and the scores obtained from them were analyzed using the average variance extracted (AVE) and composite reliability (CR) tests. The factor loadings for all items were greater than 0.5, indicating that the items converged with the relevant factor. The scores obtained for each dimension in the AVE test were greater than 0.6 and the scores for the CR test were greater than 0.75. Accordingly, seven dimensions were identified with Varimax rotation, as illustrated in the scree plot diagram (Table 4 and Figure 1).
Reliability
A re-test was performed to determine the reliability or stability of the test results. The WHODAS II was completed one week later and the results were compared. The findings showed a correlation between the questionnaire scores from one week to the next. The intraclass correlation (ICC) value was 0.84 for the 12-item questionnaire and 0.81 for the 36-item questionnaire.
The Cronbach α was used to assess internal consistency, yielding values of 0.78 and 0.62 for the 12-item and 36-item questionnaires, respectively. Additionally, the Cronbach α values less than 0.6 were not improved by removing any of the items.
Discussion
The results of the present study indicated that the Persian version of the WHODAS II has acceptable validity and reliability for assessing disability. Overall, this questionnaire demonstrates good internal consistency and can be utilized in clinical research settings involving Persian-speaking psychiatric patients.
The Cronbach α coefficient for the 36-item questionnaire was 0.788, indicating that its Persian version has good internal consistency and removing any item does not reduce the Cronbach α value below 0.7. Conversely, overall, removing item D5.3, “Do you perform all tasks related to you in the family?” from the life activities dimension, and item D5.8, “Doing occupational-educational activities as soon as possible,” also from the life activities dimension, resulted in a greater increase in the Cronbach α value compared to the removal of other items. Regarding the item “Do you perform all tasks related to you in the family?” there is a possibility that the meaning of the item is not well understood by the respondent, as the phrase “related duties” may be interpreted differently by each individual. For some, the meaning of this phrase may not be entirely clear and asking such a question may lead to resistance to providing an accurate answer.
Regarding the item “carrying out occupational-educational activities as soon as possible,” the simultaneous mention of two fields, occupation, and education, in one sentence makes it difficult for respondents to distinguish between them. People’s interpretations of the item may vary. Additionally, individuals with different jobs and educational backgrounds will likely provide various responses to this item.
Borglin et al. assessed 162 cases with physical problems and 156 cases with mental issues from 15 centers, demonstrating an acceptable internal consistency with a Cronbach α of 0.77 and a test-re-test reliability ICC of 0.74, considered acceptable [16]. The results of our study showed that the Cronbach α value for the 36-item questionnaire was 0.788. Additionally, regarding test-re-test reliability, an ICC value of 0.81 was obtained, consistent with the study’s results mentioned above. Furthermore, in another study conducted in Greece involving 10163 patients, this questionnaire demonstrated acceptable internal consistency with the version prepared in Greek [17]. Carlozzi et al. evaluated the reliability and validity of WHODAS II, which were confirmed in patients with Huntington disease [7]. In another study in Singapore involving patients with psychiatric diagnoses, the validity and reliability of this questionnaire were also confirmed [18].
Garin et al. aimed to provide a structural explanation to measure the ability and disability of patients across Europe; 1119 patients with one of 17 chronic diseases in seven medical centers were evaluated using the WHODAS II. Additionally, the patients were followed up for 6 weeks and 3 months. They reported that the WHODAS II could accurately assess disability. To establish the validity of this questionnaire, the EQ-5D was used in this study [19].
The analysis of the reliability of the 12-item questionnaire showed that the obtained Cronbach α coefficient was 0.62, which was lower than that of the 36-item questionnaire. On the other hand, the general examination of the items indicates that removing items SI, “Standing for a long time like 30 minutes,” S5, “What effect did the problems have on your emotions and feelings?” S7, “Walking long distances like 1 km,” and S8, “Washing the whole body,” might result in higher Cronbach α values than the other items. Regarding item S5, “How did the problems affect your emotions and feelings?” it is possible that respondents may not fully understand the concept of influencing emotions and feelings, leading to varying answers from different individuals.
Concerning the 36-item questionnaire, the Cronbach α values for different dimensions were as follows: Understanding and communication: 0.76; mobility: 0.69; personal hygiene: 0.78; interacting with other people: 0.72; life activities: 0.75; and participation in social activities: 0.71. Additionally, for test-re-test reliability, the ICC value was found to be 0.81, with specific values of 0.88 for understanding and communication, 0.79 for mobility, 0.77 for personal hygiene, 0.69 for interacting with other people, 0.87 for life activities and 0.81 for participation in social activities.
Conclusion
These results indicate that the questionnaire items in Persian have better reliability in the dimensions of understanding and communication, life activities, and participation in social activities. The dimensions mentioned above exhibit less variability than other dimensions and are less susceptible to significant changes over time. One of the study’s limitations was its limited number of patients and the fact that it was only conducted at two university centers. Additionally, although efforts were made to provide the necessary training to participants before filling out the questionnaire and to request that it be completed in a calm environment with sufficient mental concentration, these considerations were not feasible in some cases. It is suggested that a study with a larger sample size be conducted in several centers, involving more participants in calm conditions and with more training before completing the questionnaire. It is recommended that the Persian version developed in this research be used for research and clinical purposes.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Iran University of Medical Sciences (IR.IUMS.FMD.REC 1396.9411286008). The data were also kept confidential.
Funding
The paper was extracted from the Medical Assistant Thesis of Masoume Rafiei, approved by Iran University of Medical Sciences and financially supported by Iran University of Medical Sciences.
Authors' contributions
Conceptualization and supervision: Atefeh Ghanbari; Research, writing the original draft, review and editing: Masoumeh Rafiei and Mohammad Pir Hayati; Data collection: Masoumeh Rafiei and Mohammad Pir Khaiti: Data analysis: Mohammad Pir Khaiti; Sources: all authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to all the officials of Rasool Akram Hospital and to everyone who assisted the researchers in any way during this study.
References
- Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. 2016; 3(2):171-8. [DOI:10.1016/S2215-0366(15)00505-2] [PMID]
- Grimby G, Smedby B. ICF approved as the successor of ICIDH. J Rehabil Med. 2001; 33(5):193-4. [DOI:10.1080/165019701750419545] [PMID]
- Leonardi M, Bickenbach J, Ustun TB, Kostanjsek N, Chatterji S; MHADIE consortium. The definition of disability: What is in a name? Lancet. 2006; 368(9543):1219-21. [DOI:10.1016/S0140-6736(06)69498-1] [PMID]
- Cieza A, Stucki G. Understanding functioning, disability, and health in rheumatoid arthritis: The basis for rehabilitation care. Curr Opin Rheumatol. 2005; 17(2):183-9. [DOI:10.1097/01.bor.0000151405.56769.e4] [PMID]
- Ustün TB, Chatterji S, Kostanjsek N, Rehm J, Kennedy C, Epping-Jordan J, et al. Developing the World Health Organization disability assessment schedule 2.0. Bull World Health Organ. 2010; 88(11):815-23. [DOI:10.2471/BLT.09.067231] [PMID]
- Nasiripour AA, Tabibi J, Afkar A, Kamali M. [Effect of community based rehabilitation program implementation on disabled people living conditions in Iran (Persian)]. J Knowledge Health. 2012; 7(4):174-8. [Link]
- Carlozzi NE, Kratz AL, Downing NR, Goodnight S, Miner JA, Migliore N, et al. Validity of the 12-item World Health Organization disability assessment schedule 2.0 (WHODAS 2.0) in individuals with Huntington disease (HD). Qual Life Res. 2015; 24:1963-71. [DOI:10.1007/s11136-015-0930-x]
- Andrews G, Kemp A, Sunderland M, Von Korff M, Ustun TB. Normative data for the 12 item WHO disability assessment schedule 2.0. Plos One. 2009; 4(12):e8343. [DOI:10.1371/journal.pone.0008343] [PMID]
- Boileau NR, Stout JC, Paulsen JS, Cella D, McCormack MK, Nance MA, et al. Reliability and validity of the HD-PRO-TriadTM, a health-related quality of life measure designed to assess the symptom triad of huntington's disease. J Huntingtons Dis. 2017; 6(3):201-15. [DOI:10.3233/JHD-170238] [PMID]
- Montazeri A, Goshtasebi A, Vahdaninia M.S. [The short form health survey (SF-36): Translation and validation study of the Iranian version (Persian)]. Payesh. 2006; 5(1):49-56. [Link]
- Brazier J, Jones NA, Kind P. Testing the validity of the Euroqol and comparing it with the SF-36 health survey questionnaire. Qual Life Res. 1993; 2(3):169-80. [DOI:10.1007/BF00435221]
- Mohammadbeigi A, Mohammadsalehi N, Aligol M. Validity and reliability of the instruments and types of measurments in health applied researches. J Rafsanjan Univ Med Sci. 2015; 13(12):1153-70. [Link]
- Newman I, Lim J, Pineda F. Content validity using a mixed methods approach: Its application and development through the use of a table of specifications methodology. J Mixed Methods Res. 2013; 7(3):243-60.[DOI:10.1177/1558689813476922]
- Rangi NH, Allahyari T, Khosravi Y, Zaeri F, Saremi M. [Development of an occupational cognitive failure questionnaire (OCFQ): Evaluation validity and reliability (Persian)]. Iran Occup Health. 9(1):29-40. [Link]
- Lawshe CH. A quantitative approach to content validity. Pers psychol. 1975. 28(4):563-75. [Link]
- Borglin G, Edberg AK, Hallberg IR. The experience of quality of life among older people. J Aging Stud. 2005; 19(2):201-20. [DOI:10.1016/j.jaging.2004.04.001]
- Theotokatos G, Escorpizo R, Angelopoulos TJ, Chrysagis NK, Bickenbach J, Venieri A, et al. Psychometric properties of the 12-item World Health Organization disability assessment schedule (WHODAS 2.0), Greek version: A cross-sectional study on applicants of welfare benefits. Cureus. 2023; 15(11):e48588. [DOI:10.7759/cureus.48588] [PMID]
- Abdin E, Seet V, Jeyagurunathan A, Tan SC, Mok YM, Verma S, et al. Validation of the 12-item World Health Organization disability assessment schedule 2.0 in individuals with schizophrenia, depression, anxiety, and diabetes in singapore. Plos One. 2023; 18(11):e0294908. [DOI:10.1371/journal.pone.0294908] [PMID]
- Garin O, Ayuso-Mateos JL, Almansa J, Nieto M, Chatterji S, Vilagut G, et al. Validation of the "World Health Organization disability assessment schedule, WHODAS-2" in patients with chronic diseases. Health Qual Life Outcomes. 2010; 8:51. [DOI:10.1186/1477-7525-8-51] [PMID]
Type of Study: Research |
Subject:
Psychology
Received: 2023/10/25 | Accepted: 2023/12/17 | Published: 2024/01/1
Received: 2023/10/25 | Accepted: 2023/12/17 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
