Wed, May 27, 2026
[Archive]
Volume 1, Issue 2 (Winter 2023)
CPR 2023, 1(2): 244-261 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hajipour L, Hosseini Tabaghdehi M. Investigating the Effects of Prenatal Education on the Quality of Life (QoL) of Nulliparous Women. CPR 2023; 1 (2) :244-261
URL: http://cpr.mazums.ac.ir/article-1-44-en.html
URL: http://cpr.mazums.ac.ir/article-1-44-en.html



Department of Midwifery, Faculty of Medical Sciences, Tonekabon Branch, Islamic Azad University, Tonekabon, Iran.
Full-Text [PDF 1821 kb]
(848 Downloads)
| Abstract (HTML) (2340 Views)
Full-Text: (1152 Views)
Introduction
Pregnancy is associated with significant changes in the mental and physical health of women. The social performance of pregnant women is lower than other people in society. Even in natural pregnancy, these changes can disrupt the abilities of women. Most pregnant women, especially nulliparous mothers, have many fears and concerns. They are anxious about how to adapt themselves to their new circumstances. Accordingly, the quality of life (QoL) in pregnant women is lower compared to non-pregnant women [1, 2].
The QoL involves different dimensions of physical, mental, and social health. Measuring the QoL is important in planning for taking care of pregnant mothers and understanding their need for such care in the healthcare community [3, 4]. Knowing the QoL of individuals, identifying factors that reduce their QoL, and efforts to eliminate these barriers can improve the quality of services along with the QoL throughout the country [4]. Women, especially nulliparous, require special care to manage pregnancy and have a pleasant and safe birth experience as they are not familiar with pregnancy and the physiological problems associated with their condition. Preparing for pregnancy, midwifery, and family support during pregnancy and childbirth play an important role in having a satisfying experience for mothers. Today, routine maternity care is not enough for mothers. The lack of knowledge and fear of unknowns lead to medical interventions and wrong decisions about the delivery method. Such healthcare methods mostly emphasize the physical problems of pregnant women and are less concerned with mental health issues and women’s QoL [5, 6]. Therefore, pre-pregnancy and physiological delivery classes are currently being held in most hospitals in the country to provide such services to pregnant mothers. In these classes, parents receive information about physical and psychological changes during pregnancy, childbirth, parenting, neuropsychological, muscular, and breathing exercises, and supportive methods in labor [6, 7]. Holding classes and providing training is an effective way to protect a pregnant mother. Confidence, satisfaction with pregnancy, active participation of family members, ability to adapt and deal with problems and acceptance of life responsibilities can improve the QoL [7]. Hence, mothers learn how to solve their problems and deal with childbirth as a solvable issue [8]. In Iran, no research has been conducted on the effect of pregnancy preparation classes on the QoL of pregnant women, and given that measuring the QoL of pregnant women is important in planning for the care of mothers and babies, the results can increase the QoL, independence, self-confidence, safe pregnancy, pleasant natural childbirth, and finally improve reproductive health. This study aims to compare the QoL in nulliparous women in two groups of pregnant women participating in childbirth classes or taking routine healthcare.
Materials and Methods
This quasi-experimental study was conducted on 93 pregnant women who were referred to Amini Langroudi Hospital from 2013 to 2015. The samples were selected using the convenience sampling method and then divided into intervention and control groups. The study of Abbaszadeh was used to estimate the sample size and given the least standard deviation in this study in terms of the general health of the QoL (94.14), the sample size was estimated at 35 cases in each group. However, this number was increased to 50 cases for both groups [6]. Of the study population, two cases were excluded from the intervention group because of preterm rupture of the membranes and placental abruption, and 5 cases were excluded from the control group as a result of preterm delivery and withdrawal from continuing with the study. Eventually, 48 cases in the intervention group and 45 cases in the control group were analyzed. Among the pregnant mothers who were referred to the hospital, 50 individuals who were interested in participating in the training classes, as well as 50 individuals who were not willing to attend the class and only wanted to receive the usual pregnancy care were invited to participate in the study (Figure 1).
 Initially, written consent to participate in the study was obtained from all the participants. Then, the questionnaires were completed by mothers in their 20th week of pregnancy. The inclusion criteria were 1) being in the age range of 18 to 35 years, 2) having a gestational age of about 20 weeks, 3) having no significant medical or obstetric problem or high-risk pregnancy, and 4) having enough literacy to complete the questionnaire. The exclusion criteria were having a high-risk pregnancy during the study and not being willing to participate in the research.
Initially, written consent to participate in the study was obtained from all the participants. Then, the questionnaires were completed by mothers in their 20th week of pregnancy. The inclusion criteria were 1) being in the age range of 18 to 35 years, 2) having a gestational age of about 20 weeks, 3) having no significant medical or obstetric problem or high-risk pregnancy, and 4) having enough literacy to complete the questionnaire. The exclusion criteria were having a high-risk pregnancy during the study and not being willing to participate in the research.
Study instruments
The research tools were the personal and obstetrics information form along with the QoL questionnaire (36-item short-form survey). The questionnaires were completed by the participants of both groups in the research.
Personal and obstetric form
The personal and obstetric form collects information on the participants’ age, school education, job, and gestational age.
The QoL questionnaire
This questionnaire contains 36 questions in 8 dimensions, including physical functioning, functional limitations because of physical problems, body pain, general health, mental health, the feeling of vitality, functional limitation because of psychological problems, and social function. The total score of the 8 dimensions ranges from 0 to 100 while higher scores indicate a better situation [4, 7, 9].
The validity and reliability of the Persian version of the QoL questionnaire were approved by the Iranian Institute for Health Sciences Research [10].
Pregnant women who willingly participated in the study received pregnancy classes (intervention group) and the rest of the participants (control group) received the usual prenatal care (limited to regular examinations, routine tests, and ultrasound). The pregnant women in the intervention group were trained in 8 sessions by midwives who had previously completed the courses. Each session was formed in 3 parts within 90 min.
Part 1
The first part included training on the anatomic and physiologic changes during pregnancy, health, and nutrition during pregnancy, various stages of delivery, maternal and neonatal health, encouragement for breastfeeding, and family planning (theoretical training using audiovisual equipment).
Part 2
The second part included consultation in the form of questions and answers.
Part 3
The third part included nervous and muscular exercises, proper conditions during labor and delivery, correct breathing during pregnancy, labor, and delivery, and relaxation. Meanwhile, in the last session, mothers got familiar with the delivery room, labor room, childbirth, tools, and personnel [11, 12].
The data were analyzed via SPSS software, version 19. We used the independent t-test, the paired t-test, and the Chi-square test. The normality of the data was determined via the Kolmogorov-Smirnov test; accordingly, the data had a normal distribution.
Results
A total of 100 pregnant women were enrolled in the study. However, eventually, the statistical analysis was performed on 93 samples (48 cases in the intervention and 45 cases in the control group). The majority of the samples in the intervention group were in the age range of 25 to 30 years (50%). The age range in the control group was from 20 to 25 years (55%). A total of 66% in both groups had a high school education, 95% were housewives in the intervention group while 91% were housewives in the control group (Table 1).
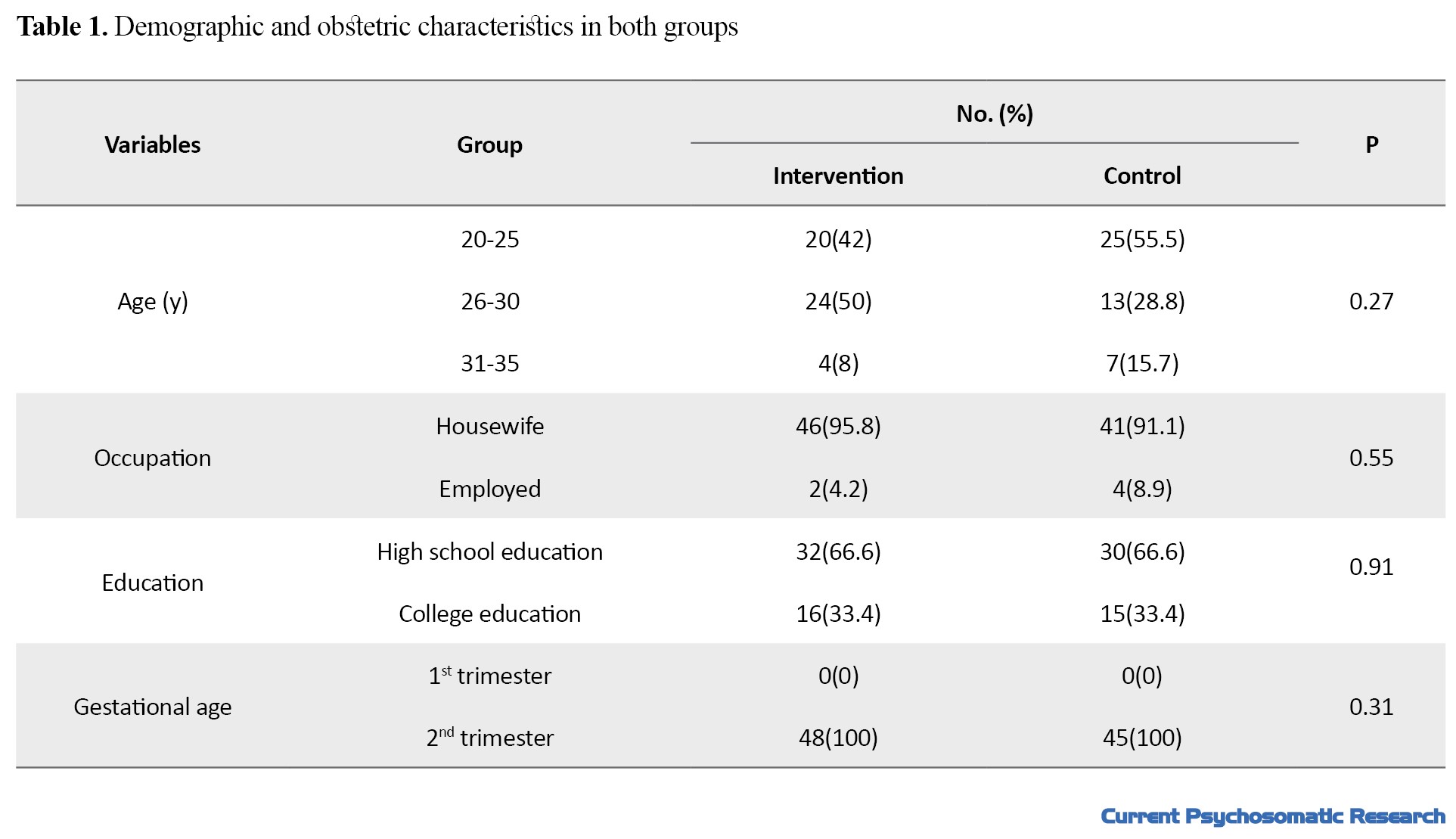
No significant difference was observed between the two groups regarding the mentioned cases when entering the study (based on the Chi-square test).
The results of the independent t-test showed no significant difference between the dimensions of life quality before the intervention in nulliparous women in both groups. In the intervention group, the dimension of social function and in the control group the dimension of body pain obtained the highest scores. The functional limitation because of physical problems had the lowest scores (Table 2).

The only significant difference was observed in the functional limitation because of physical problems between the scores of dimensions of QoL after the intervention in nulliparous women in the intervention and control groups (P=0.004). However, no statistically significant difference was observed in other dimensions (based on the independent t-test). Also, in both groups after the intervention, the mental health dimension had the highest score, and the dimension of functional limitation because of physical problems had the lowest score. The dimensions of physical function and mental health had the same health-related score. In other dimensions, except for pain, the intervention group had higher health-related performance compared to the control group (Table 2).
The comparison of Mean±SD of different dimensions of QoL in nulliparous women before and after intervention in the intervention group indicated no significant difference in 8 dimensions, except for physical function (P=0.00; paired t-test). Also, the comparison of the mean life quality dimensions in the intervention group showed that the dimensions of general health, physical function, functional limitation because of physical problems, functional limitation because of emotional problems, and social performance decreased after the intervention; however, the difference was not statistically significant. The dimensions of mental health, the feeling of vitality, and pain after the intervention had a higher health-related score compared to before the intervention, although the difference was not statistically significant (Table 3).
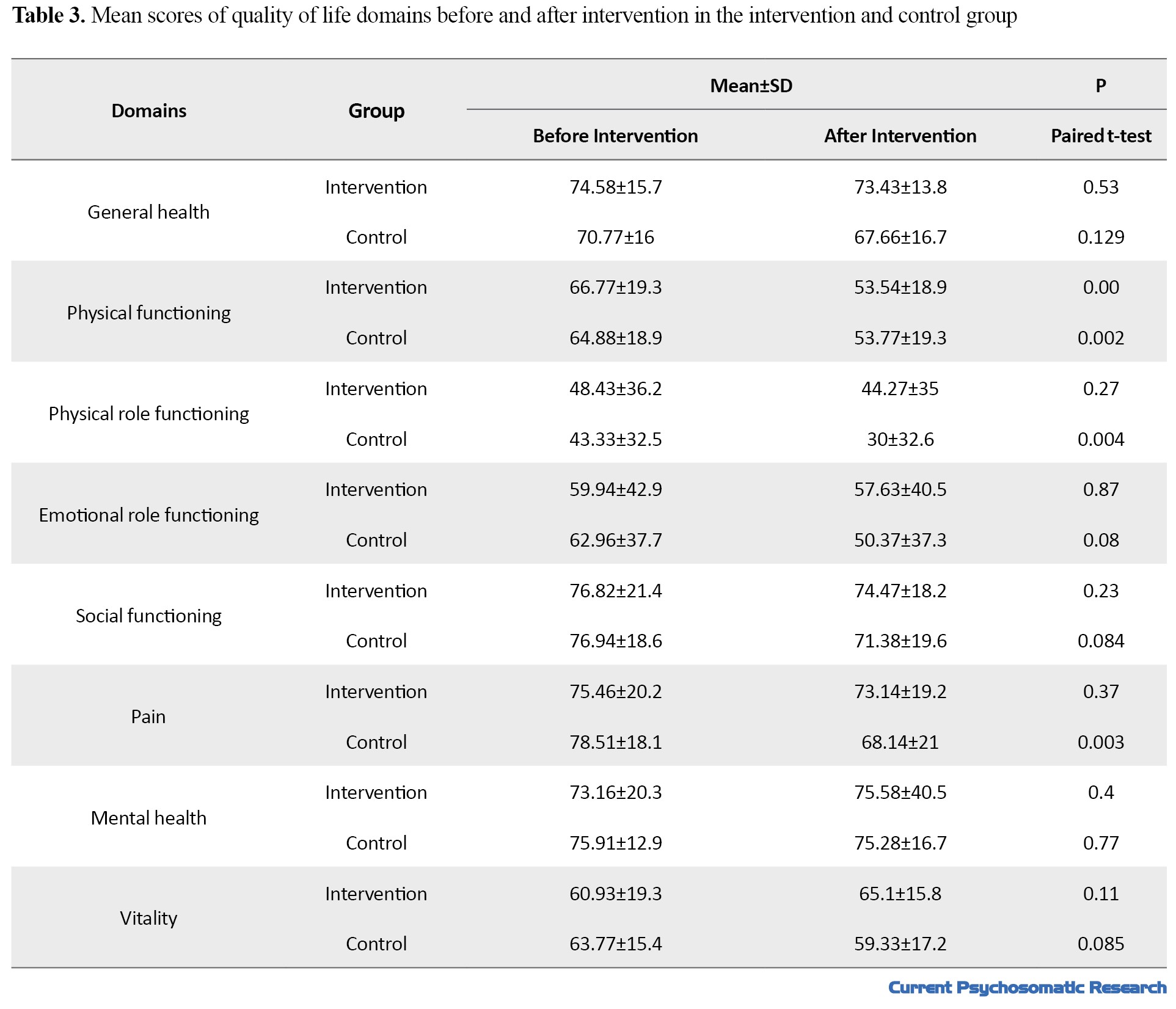
The comparison of Mean±SD of different dimensions of life quality in nulliparous women before and after class in the control group in the dimensions of physical function (P=0.002), functional limitation because of physical problems (P=0.004), and pain (P=0.003) indicated a significant difference (based on the paired t-test). The dimension of mental health had equal scores before and after the intervention. Other dimensions had lower scores after the intervention (Table 3).
Discussion
The results of this study showed no significant difference between the mean scores of the dimensions of QoL among the nulliparous women in the intervention and control groups before and after the intervention. Before and after the intervention in both groups, functional limitation because of physical problems had the lowest score, which was consistent with the studies of Abbas Zadeh and Makvandi [13, 14]. In the intervention group before the intervention, social function and the dimension of pain after the intervention had the highest scores. After intervention in both groups, mental health equally obtained the highest health-related scores. In Abbaszadeh’s study, social performance and mental health also increased [1].
Our findings showed that after training classes, mental health was better in the intervention group compared to the control group, although no significant difference was observed. In examining the differences in the dimensions of QoL in the intervention group after the intervention, a significant difference in the level of physical function, mental health, vitality, and the pain was detected which was not statistically significant. Given the hormonal and physical changes and the body’s compliance with the process of pregnancy, the pain is increased, physical and social functions are weakened, and functional limitation because of physical problems is increased [3]. The findings of the study by Karami showed that pregnancy has a negative effect on physical and social functions. Karami posited that since pregnant women have physical dysfunction, this will result in the feeling of a lack of physical health and this negatively affects their mental health. The results of Karami’s study showed a need for paying more attention to the dimension of mental health during pregnancy [1].
Changes and the incidence of problems during pregnancy such as nausea, vomiting, fatigue, and pain can have a significant effect on the daily activity of pregnant women, which can be important factors in reducing the dimensions of life quality and the woman’s ability in daily duties. The study of Makvandy showed that the lowest score is related to the feeling of vitality and functional limitation because of physical problems [14].
In the study of Abbaszadeh, conducted on 600 pregnant women, the lowest score was also attributed to the dimensions of functional limitation because of physical problems, feelings of vitality, and pain. Abbaszadeh found that the physical problems of pregnant women were higher compared to non-pregnant women and they have a lower QoL, given that they had no training course [6, 13]. In examining the differences in the dimensions of QoL in the control group, when comparing the result before and after the intervention, a significant statistical difference was observed in the physical function, functional limitations because of physical problems, and pain. Pain had decreased more significantly and the dimension of mental health had the same score before and after the intervention. Comparing the means showed a decrease in scores and a lower level of health-related function in others compared to the pre-intervention stage. Our results showed that although the dimensions of general health, physical functioning, functional limitations because of physical problems, functional limitations because of emotional problems, and social function in both groups had a downward health trend after the intervention, the intervention group, in the dimensions of mental health, pain, and feeling of vitality a higher health-related score was detected compared to before the intervention; however, the difference was not significant. Research showed that maternal support is beneficial for the mother during pregnancy to help them adapt their feelings, and also plays an important role in improving their emotional and adaptive status with motherhood roles. Pregnancy training reduces the incidence of mental disorders and depression [15, 16].
Conclusion
In the present study, the main reasons for the decreased physical function and functional limitations because of physical and emotional problems, and social function in both groups were the physiological changes during pregnancy and their progression, and perhaps the lack of good education to improve the physical condition. The psychological dimensions were better in the intervention group due to relaxing exercises and close relationships with the pregnant mother and the teacher in the classes. Therefore, healthcare providers should focus more on the symptoms and changes of pregnancy. Mothers should deal with pregnancy and childbirth as solvable and natural issues and try to improve healthy social relationships in the training classes. The results of Abbaszadeh’s study also showed that the average QoL, especially the physical and pain dimensions, decreases with the progression of pregnancy. Meanwhile, the number of pregnancies also decreases the QoL in women. In Abbaszadeh’s study, the highest mean of life quality was observed in the first pregnancy, since more pregnancies reduce the physical and mental power of women, which can negatively impact the QoL [13].
Studies showed that counseling with nulliparous women can reduce anxiety and proper education improves mothers’ awareness and enables them to use correct strategies to solve pregnancy problems [8]. Improvement in the dimensions of mental health and emotional problems following the training classes can be due to stress reduction resulting from proper training; however, with better training and increasing the sample size, better results can be obtained. The study of Pinedo also showed that pregnancy education does not have beneficial effects on pregnancy and childbirth [8]. Bahrami’s study also showed that pregnancy training classes lead to a higher life quality and a higher sense of vitality in the postpartum period. Bahrami posits that educational interventions are effective in promoting self-efficacy for delivery and lead to a reduction in pain and anxiety in labor [18].
The results of our research along with other studies indicated that the QoL of pregnant women is low; however, the low level of physical dimensions and the role limitation resulting from physical problems and even mental health can be improved by proper training and accurate healthcare during pregnancy care. Studies also showed that mothers’ support in pregnancy is beneficial in helping women to adapt to motherhood emotions and to improve their emotional state. The results of the present study indicated the role of education during pregnancy as a key element in increasing mental health [19] . In our study, the reason for the decrease in physical performance was the limitation of performance caused by physical problems and pain in both groups. Pregnancy can progress due to the increase in physical problems and pain caused by physiological changes following pregnancy and maybe the weakness in training to improve the physical condition, especially in the pregnancy preparation class in the intervention group.
Although, it is possible that mental health was better in the intervention group due to physical exercises and the close relationship between the pregnant mother and the teacher. The results of Abbaszadeh›s study show that with the progress of pregnancy, the average QoL, especially the physical dimension, and pain, decreases [6]. The results of Jakubiec ‘s study also showed that classes can improve mental health by reducing mental problems during pregnancy. It can even improve the QoL’s physical and social dimensions [20].
The improvement in mental health and emotional problems after preparation classes can be attributed to the relaxation and reduction of stress, along with proper training of the instructor; however, with more detailed training and increasing sample size, better results can be obtained.
The positive effects of relaxation in these classes can make the mother feel better and have a better QoL. Finally, delivery is a completely physiological process, and the physical and mental support of the mother is necessary to avoid any complications [15, 16].
To promote the health status of mothers who play the main role in a healthy society, more attention should be paid to the QoL during pregnancy care [19]. Also, it is necessary to conduct more studies in this field and to investigate the effect of pregnancy education on the QoL of multiparous women and maternal and neonatal health. This was a small study; thus, the results should be cautiously generalized. It is unlikely to reach a general conclusion from such a small study. The existence of cultural and social issues causes impatience and unwillingness in mothers to participate in research.
Since only the mothers who were willing to participate in the study were enrolled, the lack of random assignment is considered a research limitation. It is suggested that more studies should be carried out with a larger sample size to obtain better results and higher generalizability.
Ethical Considerations
Compliance with ethical guidelines
Samples' information was obtained after receiving written informed consent, explaining the design and its objectives, and ensuring confidentiality. A license was received from Azad University of Tonkabon branch with number 24331/1 and IRCT code 2017012732228N1.
Funding
This article is the result of a research project approved by the Islamic Azad University of Tonekabon under Contract No.: 23397 in 2012.
Authors' contributions
Conception and Supervision: leila hajipour; Collection and analysis: leila hajipour; Financial sources: Islamic Azad University of Tonekabon; Methodology and Writing and review: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Hereby, the support of the Vice-Chancellor of Research in Islamic Azad University of Tonekabon is highly appreciated. The aothors would like to thank the Guilan University of Medical Sciences, the head of Amini Langroud Hospital, and especially the cooperation of Nasrin Rahimian, who provided the opportunity to conduct this research, and all the mothers who participated in this study are sincerely appreciated.
References
Pregnancy is associated with significant changes in the mental and physical health of women. The social performance of pregnant women is lower than other people in society. Even in natural pregnancy, these changes can disrupt the abilities of women. Most pregnant women, especially nulliparous mothers, have many fears and concerns. They are anxious about how to adapt themselves to their new circumstances. Accordingly, the quality of life (QoL) in pregnant women is lower compared to non-pregnant women [1, 2].
The QoL involves different dimensions of physical, mental, and social health. Measuring the QoL is important in planning for taking care of pregnant mothers and understanding their need for such care in the healthcare community [3, 4]. Knowing the QoL of individuals, identifying factors that reduce their QoL, and efforts to eliminate these barriers can improve the quality of services along with the QoL throughout the country [4]. Women, especially nulliparous, require special care to manage pregnancy and have a pleasant and safe birth experience as they are not familiar with pregnancy and the physiological problems associated with their condition. Preparing for pregnancy, midwifery, and family support during pregnancy and childbirth play an important role in having a satisfying experience for mothers. Today, routine maternity care is not enough for mothers. The lack of knowledge and fear of unknowns lead to medical interventions and wrong decisions about the delivery method. Such healthcare methods mostly emphasize the physical problems of pregnant women and are less concerned with mental health issues and women’s QoL [5, 6]. Therefore, pre-pregnancy and physiological delivery classes are currently being held in most hospitals in the country to provide such services to pregnant mothers. In these classes, parents receive information about physical and psychological changes during pregnancy, childbirth, parenting, neuropsychological, muscular, and breathing exercises, and supportive methods in labor [6, 7]. Holding classes and providing training is an effective way to protect a pregnant mother. Confidence, satisfaction with pregnancy, active participation of family members, ability to adapt and deal with problems and acceptance of life responsibilities can improve the QoL [7]. Hence, mothers learn how to solve their problems and deal with childbirth as a solvable issue [8]. In Iran, no research has been conducted on the effect of pregnancy preparation classes on the QoL of pregnant women, and given that measuring the QoL of pregnant women is important in planning for the care of mothers and babies, the results can increase the QoL, independence, self-confidence, safe pregnancy, pleasant natural childbirth, and finally improve reproductive health. This study aims to compare the QoL in nulliparous women in two groups of pregnant women participating in childbirth classes or taking routine healthcare.
Materials and Methods
This quasi-experimental study was conducted on 93 pregnant women who were referred to Amini Langroudi Hospital from 2013 to 2015. The samples were selected using the convenience sampling method and then divided into intervention and control groups. The study of Abbaszadeh was used to estimate the sample size and given the least standard deviation in this study in terms of the general health of the QoL (94.14), the sample size was estimated at 35 cases in each group. However, this number was increased to 50 cases for both groups [6]. Of the study population, two cases were excluded from the intervention group because of preterm rupture of the membranes and placental abruption, and 5 cases were excluded from the control group as a result of preterm delivery and withdrawal from continuing with the study. Eventually, 48 cases in the intervention group and 45 cases in the control group were analyzed. Among the pregnant mothers who were referred to the hospital, 50 individuals who were interested in participating in the training classes, as well as 50 individuals who were not willing to attend the class and only wanted to receive the usual pregnancy care were invited to participate in the study (Figure 1).
Study instruments
The research tools were the personal and obstetrics information form along with the QoL questionnaire (36-item short-form survey). The questionnaires were completed by the participants of both groups in the research.
Personal and obstetric form
The personal and obstetric form collects information on the participants’ age, school education, job, and gestational age.
The QoL questionnaire
This questionnaire contains 36 questions in 8 dimensions, including physical functioning, functional limitations because of physical problems, body pain, general health, mental health, the feeling of vitality, functional limitation because of psychological problems, and social function. The total score of the 8 dimensions ranges from 0 to 100 while higher scores indicate a better situation [4, 7, 9].
The validity and reliability of the Persian version of the QoL questionnaire were approved by the Iranian Institute for Health Sciences Research [10].
Pregnant women who willingly participated in the study received pregnancy classes (intervention group) and the rest of the participants (control group) received the usual prenatal care (limited to regular examinations, routine tests, and ultrasound). The pregnant women in the intervention group were trained in 8 sessions by midwives who had previously completed the courses. Each session was formed in 3 parts within 90 min.
Part 1
The first part included training on the anatomic and physiologic changes during pregnancy, health, and nutrition during pregnancy, various stages of delivery, maternal and neonatal health, encouragement for breastfeeding, and family planning (theoretical training using audiovisual equipment).
Part 2
The second part included consultation in the form of questions and answers.
Part 3
The third part included nervous and muscular exercises, proper conditions during labor and delivery, correct breathing during pregnancy, labor, and delivery, and relaxation. Meanwhile, in the last session, mothers got familiar with the delivery room, labor room, childbirth, tools, and personnel [11, 12].
The data were analyzed via SPSS software, version 19. We used the independent t-test, the paired t-test, and the Chi-square test. The normality of the data was determined via the Kolmogorov-Smirnov test; accordingly, the data had a normal distribution.
Results
A total of 100 pregnant women were enrolled in the study. However, eventually, the statistical analysis was performed on 93 samples (48 cases in the intervention and 45 cases in the control group). The majority of the samples in the intervention group were in the age range of 25 to 30 years (50%). The age range in the control group was from 20 to 25 years (55%). A total of 66% in both groups had a high school education, 95% were housewives in the intervention group while 91% were housewives in the control group (Table 1).
No significant difference was observed between the two groups regarding the mentioned cases when entering the study (based on the Chi-square test).
The results of the independent t-test showed no significant difference between the dimensions of life quality before the intervention in nulliparous women in both groups. In the intervention group, the dimension of social function and in the control group the dimension of body pain obtained the highest scores. The functional limitation because of physical problems had the lowest scores (Table 2).
The only significant difference was observed in the functional limitation because of physical problems between the scores of dimensions of QoL after the intervention in nulliparous women in the intervention and control groups (P=0.004). However, no statistically significant difference was observed in other dimensions (based on the independent t-test). Also, in both groups after the intervention, the mental health dimension had the highest score, and the dimension of functional limitation because of physical problems had the lowest score. The dimensions of physical function and mental health had the same health-related score. In other dimensions, except for pain, the intervention group had higher health-related performance compared to the control group (Table 2).
The comparison of Mean±SD of different dimensions of QoL in nulliparous women before and after intervention in the intervention group indicated no significant difference in 8 dimensions, except for physical function (P=0.00; paired t-test). Also, the comparison of the mean life quality dimensions in the intervention group showed that the dimensions of general health, physical function, functional limitation because of physical problems, functional limitation because of emotional problems, and social performance decreased after the intervention; however, the difference was not statistically significant. The dimensions of mental health, the feeling of vitality, and pain after the intervention had a higher health-related score compared to before the intervention, although the difference was not statistically significant (Table 3).
The comparison of Mean±SD of different dimensions of life quality in nulliparous women before and after class in the control group in the dimensions of physical function (P=0.002), functional limitation because of physical problems (P=0.004), and pain (P=0.003) indicated a significant difference (based on the paired t-test). The dimension of mental health had equal scores before and after the intervention. Other dimensions had lower scores after the intervention (Table 3).
Discussion
The results of this study showed no significant difference between the mean scores of the dimensions of QoL among the nulliparous women in the intervention and control groups before and after the intervention. Before and after the intervention in both groups, functional limitation because of physical problems had the lowest score, which was consistent with the studies of Abbas Zadeh and Makvandi [13, 14]. In the intervention group before the intervention, social function and the dimension of pain after the intervention had the highest scores. After intervention in both groups, mental health equally obtained the highest health-related scores. In Abbaszadeh’s study, social performance and mental health also increased [1].
Our findings showed that after training classes, mental health was better in the intervention group compared to the control group, although no significant difference was observed. In examining the differences in the dimensions of QoL in the intervention group after the intervention, a significant difference in the level of physical function, mental health, vitality, and the pain was detected which was not statistically significant. Given the hormonal and physical changes and the body’s compliance with the process of pregnancy, the pain is increased, physical and social functions are weakened, and functional limitation because of physical problems is increased [3]. The findings of the study by Karami showed that pregnancy has a negative effect on physical and social functions. Karami posited that since pregnant women have physical dysfunction, this will result in the feeling of a lack of physical health and this negatively affects their mental health. The results of Karami’s study showed a need for paying more attention to the dimension of mental health during pregnancy [1].
Changes and the incidence of problems during pregnancy such as nausea, vomiting, fatigue, and pain can have a significant effect on the daily activity of pregnant women, which can be important factors in reducing the dimensions of life quality and the woman’s ability in daily duties. The study of Makvandy showed that the lowest score is related to the feeling of vitality and functional limitation because of physical problems [14].
In the study of Abbaszadeh, conducted on 600 pregnant women, the lowest score was also attributed to the dimensions of functional limitation because of physical problems, feelings of vitality, and pain. Abbaszadeh found that the physical problems of pregnant women were higher compared to non-pregnant women and they have a lower QoL, given that they had no training course [6, 13]. In examining the differences in the dimensions of QoL in the control group, when comparing the result before and after the intervention, a significant statistical difference was observed in the physical function, functional limitations because of physical problems, and pain. Pain had decreased more significantly and the dimension of mental health had the same score before and after the intervention. Comparing the means showed a decrease in scores and a lower level of health-related function in others compared to the pre-intervention stage. Our results showed that although the dimensions of general health, physical functioning, functional limitations because of physical problems, functional limitations because of emotional problems, and social function in both groups had a downward health trend after the intervention, the intervention group, in the dimensions of mental health, pain, and feeling of vitality a higher health-related score was detected compared to before the intervention; however, the difference was not significant. Research showed that maternal support is beneficial for the mother during pregnancy to help them adapt their feelings, and also plays an important role in improving their emotional and adaptive status with motherhood roles. Pregnancy training reduces the incidence of mental disorders and depression [15, 16].
Conclusion
In the present study, the main reasons for the decreased physical function and functional limitations because of physical and emotional problems, and social function in both groups were the physiological changes during pregnancy and their progression, and perhaps the lack of good education to improve the physical condition. The psychological dimensions were better in the intervention group due to relaxing exercises and close relationships with the pregnant mother and the teacher in the classes. Therefore, healthcare providers should focus more on the symptoms and changes of pregnancy. Mothers should deal with pregnancy and childbirth as solvable and natural issues and try to improve healthy social relationships in the training classes. The results of Abbaszadeh’s study also showed that the average QoL, especially the physical and pain dimensions, decreases with the progression of pregnancy. Meanwhile, the number of pregnancies also decreases the QoL in women. In Abbaszadeh’s study, the highest mean of life quality was observed in the first pregnancy, since more pregnancies reduce the physical and mental power of women, which can negatively impact the QoL [13].
Studies showed that counseling with nulliparous women can reduce anxiety and proper education improves mothers’ awareness and enables them to use correct strategies to solve pregnancy problems [8]. Improvement in the dimensions of mental health and emotional problems following the training classes can be due to stress reduction resulting from proper training; however, with better training and increasing the sample size, better results can be obtained. The study of Pinedo also showed that pregnancy education does not have beneficial effects on pregnancy and childbirth [8]. Bahrami’s study also showed that pregnancy training classes lead to a higher life quality and a higher sense of vitality in the postpartum period. Bahrami posits that educational interventions are effective in promoting self-efficacy for delivery and lead to a reduction in pain and anxiety in labor [18].
The results of our research along with other studies indicated that the QoL of pregnant women is low; however, the low level of physical dimensions and the role limitation resulting from physical problems and even mental health can be improved by proper training and accurate healthcare during pregnancy care. Studies also showed that mothers’ support in pregnancy is beneficial in helping women to adapt to motherhood emotions and to improve their emotional state. The results of the present study indicated the role of education during pregnancy as a key element in increasing mental health [19] . In our study, the reason for the decrease in physical performance was the limitation of performance caused by physical problems and pain in both groups. Pregnancy can progress due to the increase in physical problems and pain caused by physiological changes following pregnancy and maybe the weakness in training to improve the physical condition, especially in the pregnancy preparation class in the intervention group.
Although, it is possible that mental health was better in the intervention group due to physical exercises and the close relationship between the pregnant mother and the teacher. The results of Abbaszadeh›s study show that with the progress of pregnancy, the average QoL, especially the physical dimension, and pain, decreases [6]. The results of Jakubiec ‘s study also showed that classes can improve mental health by reducing mental problems during pregnancy. It can even improve the QoL’s physical and social dimensions [20].
The improvement in mental health and emotional problems after preparation classes can be attributed to the relaxation and reduction of stress, along with proper training of the instructor; however, with more detailed training and increasing sample size, better results can be obtained.
The positive effects of relaxation in these classes can make the mother feel better and have a better QoL. Finally, delivery is a completely physiological process, and the physical and mental support of the mother is necessary to avoid any complications [15, 16].
To promote the health status of mothers who play the main role in a healthy society, more attention should be paid to the QoL during pregnancy care [19]. Also, it is necessary to conduct more studies in this field and to investigate the effect of pregnancy education on the QoL of multiparous women and maternal and neonatal health. This was a small study; thus, the results should be cautiously generalized. It is unlikely to reach a general conclusion from such a small study. The existence of cultural and social issues causes impatience and unwillingness in mothers to participate in research.
Since only the mothers who were willing to participate in the study were enrolled, the lack of random assignment is considered a research limitation. It is suggested that more studies should be carried out with a larger sample size to obtain better results and higher generalizability.
Ethical Considerations
Compliance with ethical guidelines
Samples' information was obtained after receiving written informed consent, explaining the design and its objectives, and ensuring confidentiality. A license was received from Azad University of Tonkabon branch with number 24331/1 and IRCT code 2017012732228N1.
Funding
This article is the result of a research project approved by the Islamic Azad University of Tonekabon under Contract No.: 23397 in 2012.
Authors' contributions
Conception and Supervision: leila hajipour; Collection and analysis: leila hajipour; Financial sources: Islamic Azad University of Tonekabon; Methodology and Writing and review: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Hereby, the support of the Vice-Chancellor of Research in Islamic Azad University of Tonekabon is highly appreciated. The aothors would like to thank the Guilan University of Medical Sciences, the head of Amini Langroud Hospital, and especially the cooperation of Nasrin Rahimian, who provided the opportunity to conduct this research, and all the mothers who participated in this study are sincerely appreciated.
References
- Karami Kh, Mardani A. [Relationship between mental health and quality of life in pregnant women (Persian)]. Q J Health Breeze. 2014; 2(1):10-7. [Link]
- Kasemi F, Nahidi F, Kariman N. Assessment scale, associated factores and quality of life score in pregnant women in Iran. Glob J Health Sci. 2016; 8(11). [DOI:10.5539/gjhs.v8n11p127]
- Zahedi M, Deris F. [Quality of life in pregnant women in farokhshar city, 2012 (Persian)]. J Clin Nur Midwifery. 2014; 3(3):63-9. [DOI:10.17795/nmsjournal17987]
- Torkan B, Parsay S, Lamyian M, Kazemnejad A, Montazeri A. Postnatal quality of life in women after normal vaginal delivery and caesarean section. BMC Pregnancy Childbirth. 2009; 9:4. [DOI:10.1186/1471-2393-9-4] [PMID] [PMCID]
- Jafari E, Mohebi P, Sedaghatpisheh T, Mazloomzadeh S. [Comparison of personal Control and its related factors pain and labor outcoms in physiological and and routine childbirth groups (Persian)]. J RafsanjanUniv Med Sci. 2016; 14(12):1033-48. [Link]
- Abbaszadh F, Baghery A, Mehran NA. [Quality of life in pregnant women (Persian)]. J Hayat. 2009; 15(1):41-8. [Link]
- Hajipour L, Mohtasham Amiri Z, Montazeri A, Torkan B, Hosseini Tabaghdehi M. The effects of prenatal classes on the quality of life in pregnant women. J Holistic Nurs Midwifery. 2017; 27(1):45-51. [DOI:10.18869/acadpub.hnmj.27.1.45]
- Delaram M, Soltanpour F. [The effect of counseling in third tiramester on anxiety of nuliparous women at the time of admission for labor (Persian)]. Zahedan J Res Med Sci. 2012; 14(2):e93584. [Link]
- Bahrami N, Bahrami S. [The survey of quality of life in first-time women in postpartum period (Persian)]. Iran J Nurs Res. 2011; 6(23):59-64. [Link]
- Montazeri A, Goshtasebi A, Vahdaninia M. [Short Form Health Survey ( SF-36): Translation and validation study of the Iranian version (Persian)]. Payesh. 2005; 5(1):49-56. [Link]
- Firuzbakhat M, Nikpour M, Asadi S. [The effect of prenatal education classes on the process of delivery (Persian)]. J Health Breeze. 2014; 2(1):45-52. [Link]
- Mehdizadeh A, Roosta F, kamali Z, Khoshgoo N. [Evaluation of the Antenatal preparation for Childbirth courses on the health of mother & the newborn (Persian)]. Journal of Iran University of Medical Sceince. 2002; 10(35):455-62. [Link]
- Abbaszadh F, Bagheri A, Mehran N. [Quality of life in pregnant women (Persian)]. Payesh . 2010; 9(1):69-75. [Link]
- Makvandi S, Etemadi kermani A. [Quality of life of pregnant women referred to health centers in Izeh (2010) (Persian)]. Kermanshah Univ Med Sci. 2012; 16(1):e78880. [Link]
- Akbarzadeh M, Toosi M, Zare N, Sharif F. [The effect of relaxation education on Mother ,s quality of life and intensity of worry after delivery (Persian)]. Danesh and Tandurusty. 2012; 7(2):83-8. [Link]
- Mehrabadi M, Mortazavi F, Rakhshani MH. Examining the effect of attending childbirth preparation classes on prepartum and postpartum maternal mental well-being index. Journal of Obstetrics, Gynecology and Cancer Research, 2022; 4(2):69-74. [DOI:10.30699/jogcr.4.2.69]
- Artieta-Pinedo I, Paz-Pascual C, Grandes G, Remiro-Fernandezdegamboa G, Odriozola-Hermosilla I, Bacigalupe A, et al. The benefits of antenatal education for the childbirth process in Spain. Nurs Res. 2010; 59(3):194-202. [DOI:10.1097/NNR.0b013e3181dbbb4e] [PMID]
- Bahrami N, Simbar M, Bahrami S.The effect of prenatal education on mother's quality of life during first year postpartum among Iranian women: A randomized controlled trial. Int J Fertil Steril. 2013; 7(3):169-74. [PMID]
- Lagadec N, Steinecker M, Kapassi A, Magnier AM, Chastang J, Robert S, et al. Factors influencing the quality of life of pregnant women: A systematic review. BMC Pregnancy Childbirth. 2018; 18(1):455. [DOI:10.1186/s12884-018-2087-4] [PMID] [PMCID]
- Jakubiec D, Jagielska K, Karmowski M, Kubicka K, Karmowski A, Sobiech KA. Effect of attending chilbbirth eduction classes on psychological distress in pregnant women measured by means of the General Health Questionnaire. Adv Clin Exp Med. 2014; 23(6):953-7. [PMID]
Type of Study: Applicable |
Subject:
Midwifery
Received: 2022/12/19 | Accepted: 2023/03/9 | Published: 2023/01/30
Received: 2022/12/19 | Accepted: 2023/03/9 | Published: 2023/01/30
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
