Wed, May 27, 2026
[Archive]
Volume 1, Issue 1 (Autumn 2022)
CPR 2022, 1(1): 116-129 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Talebi E, Rabiepoor S, Shahhosseini Z, Hosseini Tabaghdehi M. Investigating the Sexual Quality of Life of Deaf and Hard-ofHearing Married Women: A Cross-sectional Study. CPR 2022; 1 (1) :116-129
URL: http://cpr.mazums.ac.ir/article-1-37-en.html
URL: http://cpr.mazums.ac.ir/article-1-37-en.html



Department of Midwifery, Health Reproductive Research Center, Sari Branch, Islamic Azad University, Sari, Iran.
Full-Text [PDF 1604 kb]
(777 Downloads)
| Abstract (HTML) (1996 Views)
Full-Text: (3723 Views)
Introduction
Hearing impairment is the most common chronic sensory disorder in adults worldwide [1]. This impairment has important consequences on people's quality of life (QoL). Approximately 3.5% of the world's population (360 million people) suffers from disabling hard-of-hearing most people with this problem live in low- or middle-income countries [2]. Many deaf people manage to start a family like normal people. Family can be a place for their further growth and having their children. Based on proper family relations, couples' intimacy and marriage can affect happiness or marital conflicts [3]. Performing husband duties to support a wife helps maintain family relations and failure to perform them leads to the disintegration of the family [4].
One of the crucial physical and mental dimensions of women's QoL is the dimension of their sexual life, which is influenced by many individual factors and has a decisive role in women's life and health [5]. Women's sexual QoL is one of the key issues in the field of sexual health and reproduction [6]. It includes people's evaluation of the positive and negative aspects of sexual relations and responses to these evaluations [7, 8]. The sexual QoL is a tool to examine the relationship between sexual problems and QoL [9]. In other words, the sexual QoL is a measure of success and marital performance that predicts the continuity and stability of marriage and is one of the main issues in sexual health and productivity [10]. Therefore, measuring the sexual QoL is a critical issue in evaluating the short-term and long-term consequences of sexual problems [1]. Loss or decrease in sexual satisfaction can lead to symptoms of depression, marital conflicts, separation, and divorce. Chronic stress caused by marital conflicts can also cause heart disease, diabetes, and cancer [11]. Impaired sexual health and reduced quality of sexual life harm people's self-esteem and satisfaction [12]. Holmberg et al. found that the quality of sexual life is a significant predictor of mental and sexual health [13].
The international community and governments are trying to reduce the negative consequences of poor sexual health and reproduction. The international conference on population and development (ICPD) in Cairo in 1994 called on developing measures to raise awareness of disability issues and advocated for improved access to education, training, and rehabilitation services for people with disabilities. In addition, he called on governments to eradicate all forms of discrimination faced by persons with disabilities so that they can use their sexual and reproductive rights [14].
However, negative perceptions of disability and a lack of societal understanding of their concerns have hindered efforts to improve access to sexual and reproductive health services. The traditional view of disability as a medical condition or defect perpetuates negative perceptions of the abilities of people with disabilities. This representation of disability has affected the access of people with disabilities to social and economic opportunities [15]. In terms of gender and sexuality, people with disabilities are not considered sexually active as a result of their disability and often excluded from programs related to sexual health issues. Therefore, people with disabilities probably have sexual health and reproductive problems, even worse than people without disabilities, while they often receive inadequate services [16].
Deafness may cause communication problems with significant consequences for the cognitive, social, and emotional well-being of affected people. Considering the importance of the above issues, little information is available about the sexual QoL of deaf and hard-of-hearing people, especially women in our country, which can be used to design special interventions related to health. Therefore, this study examines the sexual QoL of deaf and hard of hearing married women in Mazandaran Province, Sari City, Iran.
Materials and Method
The current cross-sectional descriptive study was conducted on 132 deaf, and hard-of-hearing women referred to the Deaf Center in Mazandaran Province, Sari City, Iran, from July to November 2021. Sampling was done using the convenience method among all married women with hearing impairment referred to that center. The inclusion criteria were as follows: having a hearing impairment, being married, and having a husband alive. In this study, all participants could withdraw from filling out the questionnaire whenever they wanted, and they were informed that their information would only be available to the senior researcher. They completed the informed consent form to participate in the research.
Study tools
The research tools were the demographic form and the questionnaires on the sexual QoL-female. The questionnaires were completed by an inexperienced interviewer familiar with the sign language of the deaf in a quiet space.
Demographic form
This form collects information on the participant’s age, education, job, husband's employment status, the hearing status of self and husband, duration of the marriage, menstrual status, type of contraceptive method, history of breastfeeding, number of pregnancies, abortion, type of childbirth and participation in virtual groups of reproductive health.
The sexual QoL-female questionnaire
This questionnaire is a self-report measure to evaluate the effect of sexual disorders on the QoL of women. It measures the quality of women's sexual life in 4 areas: sexual, psychological feeling, sexual satisfaction, self-worthlessness, and sexual suppression. This tool was presented for the first time in 1998 and was reviewed and validated in 2005 by Simmonds and colleagues. It consists of 18 questions. The first field includes 7 questions (2, 3, 7, 8, 10, 16, and 17), the second field 5 questions (1, 5, 9, 13, and 18), the third field 3 questions (4, 6, and 15) and the fourth field 3 questions (11, 12, and 14). Rach item is scored on a 6-point Likert scale (strongly agree to strongly disagree). Answers are graded from 1 to 6. The total score is obtained from 18 to 108, and a higher score indicates a more favorable sexual QoL [17]. The validity and reliability of this tool for Iranian women were validated by Masoumi et al. and the internal consistency of this tool was confirmed with an alpha index of 95% [18].
In this study, mean and standard deviation were used to describe quantitative variables, and number and percentage to describe qualitative variables under SPSS software , version 24. Also, to examine the relationship between variables, the univariate analysis included a 2-independent t test and 1-way analysis of variance (ANOVA) were used. A significance level of less than 0.05 was considered.
Results
According to the study findings, the Mean±SD of the participant's age was 36.45±7.17 years, their husbands’ was 39.52±7.45 years, and their marriage durations’ was 21.87±5.40. In this study, 27 people (20.7%) participated in reproductive health virtual groups. Table 1 presents other demographic and reproductive characteristics of the participants.
.jpg)
The average score of the sexual QoL of deaf and hard-of-hearing women obtained in this study was 86.83±16.67 (minimum 35 and maximum 108) (Table 2).
.jpg)
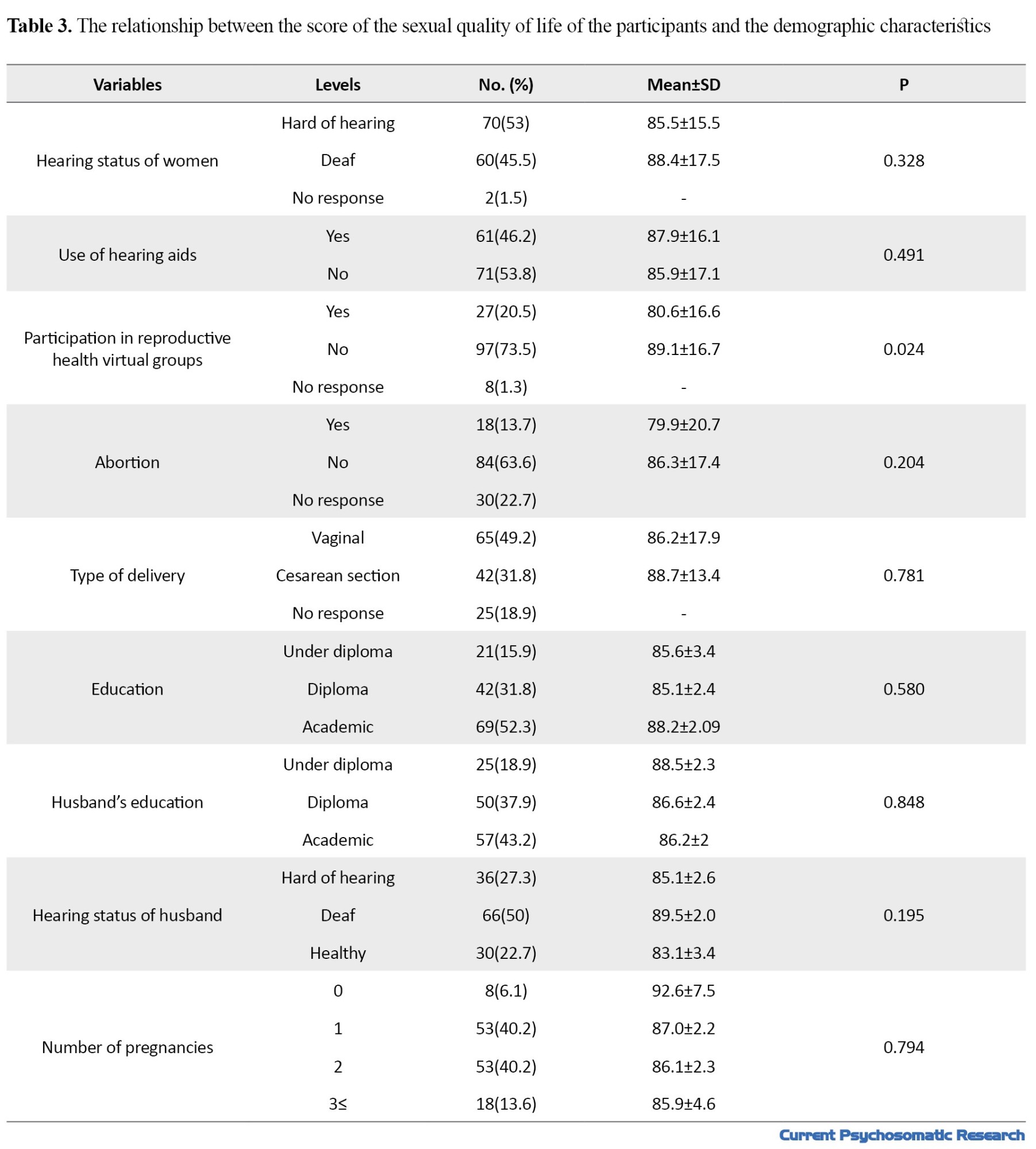
A significant relationship was observed between the sexual QoL of the samples and participating in reproductive health virtual groups (t=-2.290, P=0.024). No significant relationship was observed about other variables, such as education, husband’s education, husband’s hearing status, participants’ hearing status, use of hearing aids, number of pregnancies, type of pregnancy, type of childbirth, and history of abortion (Table 3).
Discussion
In this study, the average sexual QoL of deaf women is 83.86. In Masoumi et al.’s study on 100 married women, the average sexual quality of women’s life was 86.4 [18]. Comparing the average sexual QoL of deaf people with normal people shows that other sensory factors, such as the sense of sight play a more effective role concerning the desired sexual performance. It is suggested to use visual and other methods to improve the sexual QoL of deaf women. In this regard, Koenberg et al. study showed that providing powerful and visually accessible communication through sign language is an integral approach to health promotion [19]. In this study, although the average score is higher than the median, due to the small number of studies in this field, it is required to study more with women with different disabilities and compare their results.
According to the present study, about 21% of the samples participated in reproductive health virtual groups and had a lower sexual QoL. Contrary to the above findings, Kuenberg showed that the use of communication technologies had an effective role in improving the health of deaf women [19]. From the above results, one of the possible reasons for to decrease in the sexual QoL in these women can be the creation of unrealistic expectations in women. As a result, their husbands do not understand their needs well that ends in a disturbance in the understanding and satisfaction of their sexual activity.
The present study also showed that the quality of sexual life of deaf people had no significant relationship with women’seducation, husband’s education, type of delivery, abortion, and the number of women’s pregnancies. Although no study has been conducted in this regard, the results of studies related to the QoL of deaf people showed that the consequences of hearing loss are different from one person to another and harm the QoL, especially from the psychological aspect, social functioning and general health [20].
In this study, the descriptive results of variables, such as the use of contraceptive methods and breastfeeding status, which reflect the reproductive and sexual health status of deaf and hard-of-hearing women, show that the current situation is far from the ideal situation. This situation requires a study in the field of identifying obstacles to deaf women’s access to health services in our country. Consistent with this issue, a review study was conducted by Komori, in which education, interpersonal relations, cultural, social, and economic factors were mentioned as barriers to deaf women’s access to health services [21]. Since sexual function is one of the crucial dimensions of human life and is influenced by many factors, such as individual characteristics, interpersonal relationships, family, social, cultural, mental, and hormonal health conditions, it is recommended to conduct studies with more samples and diverse conditions.
This study also had some limitations. In this research, due to the sexual topic of the research, the shyness of women in expressing personal issues in life, the possibility of non-response or wrong answer to the options was not far from expected. Another limitation that could cause non-response or incorrect answers was the limited vocabulary in sign language. So, it is recommended that a special questionnaire be designed for the deaf to understand the questions in future studies better. Among other limitations, few studies have been conducted in the field of investigating the variables related to the quality of sexual life in deaf women. Therefore, the authors of this article were forced to compare the quality of sexual life with normal women to compare with previous research studies.
According to the study results, and the lack of providing health information in sign language for deaf people, health policies should consider and support peer-based education and the training of sign language interpreters to promote sexual and reproductive health.
Conclusion
According to the study results, and the lack of providing health information in sign language for deaf people, health policies should consider and support peer-based education and the training of sign language interpreters to promote sexual and reproductive health.
Ethical Considerations
Compliance with ethical guidelines
Information was obtained from the samples after receiving informed written consent, explaining the design and its objectives, and ensuring confidentiality. The code of ethics was obtained from Mazandaran University of Medical Sciences (IR.MAZUMS..REC.1399.403).
Funding
This project (No.: 7700) was carried out with the full support and funding of Mazandaran University of Medical Sciences and the Sexual Health and Fertility Research Center of Mazandaran University of Medical Sciences.
Authors' contributions
Conceptualization and Supervision: Erfaneh Talebi and Zohreh Shahhosseini; Methodology: Zohreh Shahhosseini and Soheila Rabiepoor; Data collection: Erfaneh Talebi and Zohreh Shahhosseini; Data analysis: Zohreh Shahhosseini and Monirolsadate Hosseini-Tabaghdehi; Funding acquisition and Resources: Erfaneh Talebi and Zohreh Shahhosseini. Investigation, Writing–original draft, and Writing-review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We express our gratitude to Mazandaran University of Medical Sciences for the financial support of this project (project number 7700) and all the participants who helped us conduct the research.
References
Hearing impairment is the most common chronic sensory disorder in adults worldwide [1]. This impairment has important consequences on people's quality of life (QoL). Approximately 3.5% of the world's population (360 million people) suffers from disabling hard-of-hearing most people with this problem live in low- or middle-income countries [2]. Many deaf people manage to start a family like normal people. Family can be a place for their further growth and having their children. Based on proper family relations, couples' intimacy and marriage can affect happiness or marital conflicts [3]. Performing husband duties to support a wife helps maintain family relations and failure to perform them leads to the disintegration of the family [4].
One of the crucial physical and mental dimensions of women's QoL is the dimension of their sexual life, which is influenced by many individual factors and has a decisive role in women's life and health [5]. Women's sexual QoL is one of the key issues in the field of sexual health and reproduction [6]. It includes people's evaluation of the positive and negative aspects of sexual relations and responses to these evaluations [7, 8]. The sexual QoL is a tool to examine the relationship between sexual problems and QoL [9]. In other words, the sexual QoL is a measure of success and marital performance that predicts the continuity and stability of marriage and is one of the main issues in sexual health and productivity [10]. Therefore, measuring the sexual QoL is a critical issue in evaluating the short-term and long-term consequences of sexual problems [1]. Loss or decrease in sexual satisfaction can lead to symptoms of depression, marital conflicts, separation, and divorce. Chronic stress caused by marital conflicts can also cause heart disease, diabetes, and cancer [11]. Impaired sexual health and reduced quality of sexual life harm people's self-esteem and satisfaction [12]. Holmberg et al. found that the quality of sexual life is a significant predictor of mental and sexual health [13].
The international community and governments are trying to reduce the negative consequences of poor sexual health and reproduction. The international conference on population and development (ICPD) in Cairo in 1994 called on developing measures to raise awareness of disability issues and advocated for improved access to education, training, and rehabilitation services for people with disabilities. In addition, he called on governments to eradicate all forms of discrimination faced by persons with disabilities so that they can use their sexual and reproductive rights [14].
However, negative perceptions of disability and a lack of societal understanding of their concerns have hindered efforts to improve access to sexual and reproductive health services. The traditional view of disability as a medical condition or defect perpetuates negative perceptions of the abilities of people with disabilities. This representation of disability has affected the access of people with disabilities to social and economic opportunities [15]. In terms of gender and sexuality, people with disabilities are not considered sexually active as a result of their disability and often excluded from programs related to sexual health issues. Therefore, people with disabilities probably have sexual health and reproductive problems, even worse than people without disabilities, while they often receive inadequate services [16].
Deafness may cause communication problems with significant consequences for the cognitive, social, and emotional well-being of affected people. Considering the importance of the above issues, little information is available about the sexual QoL of deaf and hard-of-hearing people, especially women in our country, which can be used to design special interventions related to health. Therefore, this study examines the sexual QoL of deaf and hard of hearing married women in Mazandaran Province, Sari City, Iran.
Materials and Method
The current cross-sectional descriptive study was conducted on 132 deaf, and hard-of-hearing women referred to the Deaf Center in Mazandaran Province, Sari City, Iran, from July to November 2021. Sampling was done using the convenience method among all married women with hearing impairment referred to that center. The inclusion criteria were as follows: having a hearing impairment, being married, and having a husband alive. In this study, all participants could withdraw from filling out the questionnaire whenever they wanted, and they were informed that their information would only be available to the senior researcher. They completed the informed consent form to participate in the research.
Study tools
The research tools were the demographic form and the questionnaires on the sexual QoL-female. The questionnaires were completed by an inexperienced interviewer familiar with the sign language of the deaf in a quiet space.
Demographic form
This form collects information on the participant’s age, education, job, husband's employment status, the hearing status of self and husband, duration of the marriage, menstrual status, type of contraceptive method, history of breastfeeding, number of pregnancies, abortion, type of childbirth and participation in virtual groups of reproductive health.
The sexual QoL-female questionnaire
This questionnaire is a self-report measure to evaluate the effect of sexual disorders on the QoL of women. It measures the quality of women's sexual life in 4 areas: sexual, psychological feeling, sexual satisfaction, self-worthlessness, and sexual suppression. This tool was presented for the first time in 1998 and was reviewed and validated in 2005 by Simmonds and colleagues. It consists of 18 questions. The first field includes 7 questions (2, 3, 7, 8, 10, 16, and 17), the second field 5 questions (1, 5, 9, 13, and 18), the third field 3 questions (4, 6, and 15) and the fourth field 3 questions (11, 12, and 14). Rach item is scored on a 6-point Likert scale (strongly agree to strongly disagree). Answers are graded from 1 to 6. The total score is obtained from 18 to 108, and a higher score indicates a more favorable sexual QoL [17]. The validity and reliability of this tool for Iranian women were validated by Masoumi et al. and the internal consistency of this tool was confirmed with an alpha index of 95% [18].
In this study, mean and standard deviation were used to describe quantitative variables, and number and percentage to describe qualitative variables under SPSS software , version 24. Also, to examine the relationship between variables, the univariate analysis included a 2-independent t test and 1-way analysis of variance (ANOVA) were used. A significance level of less than 0.05 was considered.
Results
According to the study findings, the Mean±SD of the participant's age was 36.45±7.17 years, their husbands’ was 39.52±7.45 years, and their marriage durations’ was 21.87±5.40. In this study, 27 people (20.7%) participated in reproductive health virtual groups. Table 1 presents other demographic and reproductive characteristics of the participants.
The average score of the sexual QoL of deaf and hard-of-hearing women obtained in this study was 86.83±16.67 (minimum 35 and maximum 108) (Table 2).
A significant relationship was observed between the sexual QoL of the samples and participating in reproductive health virtual groups (t=-2.290, P=0.024). No significant relationship was observed about other variables, such as education, husband’s education, husband’s hearing status, participants’ hearing status, use of hearing aids, number of pregnancies, type of pregnancy, type of childbirth, and history of abortion (Table 3).
Discussion
In this study, the average sexual QoL of deaf women is 83.86. In Masoumi et al.’s study on 100 married women, the average sexual quality of women’s life was 86.4 [18]. Comparing the average sexual QoL of deaf people with normal people shows that other sensory factors, such as the sense of sight play a more effective role concerning the desired sexual performance. It is suggested to use visual and other methods to improve the sexual QoL of deaf women. In this regard, Koenberg et al. study showed that providing powerful and visually accessible communication through sign language is an integral approach to health promotion [19]. In this study, although the average score is higher than the median, due to the small number of studies in this field, it is required to study more with women with different disabilities and compare their results.
According to the present study, about 21% of the samples participated in reproductive health virtual groups and had a lower sexual QoL. Contrary to the above findings, Kuenberg showed that the use of communication technologies had an effective role in improving the health of deaf women [19]. From the above results, one of the possible reasons for to decrease in the sexual QoL in these women can be the creation of unrealistic expectations in women. As a result, their husbands do not understand their needs well that ends in a disturbance in the understanding and satisfaction of their sexual activity.
The present study also showed that the quality of sexual life of deaf people had no significant relationship with women’seducation, husband’s education, type of delivery, abortion, and the number of women’s pregnancies. Although no study has been conducted in this regard, the results of studies related to the QoL of deaf people showed that the consequences of hearing loss are different from one person to another and harm the QoL, especially from the psychological aspect, social functioning and general health [20].
In this study, the descriptive results of variables, such as the use of contraceptive methods and breastfeeding status, which reflect the reproductive and sexual health status of deaf and hard-of-hearing women, show that the current situation is far from the ideal situation. This situation requires a study in the field of identifying obstacles to deaf women’s access to health services in our country. Consistent with this issue, a review study was conducted by Komori, in which education, interpersonal relations, cultural, social, and economic factors were mentioned as barriers to deaf women’s access to health services [21]. Since sexual function is one of the crucial dimensions of human life and is influenced by many factors, such as individual characteristics, interpersonal relationships, family, social, cultural, mental, and hormonal health conditions, it is recommended to conduct studies with more samples and diverse conditions.
This study also had some limitations. In this research, due to the sexual topic of the research, the shyness of women in expressing personal issues in life, the possibility of non-response or wrong answer to the options was not far from expected. Another limitation that could cause non-response or incorrect answers was the limited vocabulary in sign language. So, it is recommended that a special questionnaire be designed for the deaf to understand the questions in future studies better. Among other limitations, few studies have been conducted in the field of investigating the variables related to the quality of sexual life in deaf women. Therefore, the authors of this article were forced to compare the quality of sexual life with normal women to compare with previous research studies.
According to the study results, and the lack of providing health information in sign language for deaf people, health policies should consider and support peer-based education and the training of sign language interpreters to promote sexual and reproductive health.
Conclusion
According to the study results, and the lack of providing health information in sign language for deaf people, health policies should consider and support peer-based education and the training of sign language interpreters to promote sexual and reproductive health.
Ethical Considerations
Compliance with ethical guidelines
Information was obtained from the samples after receiving informed written consent, explaining the design and its objectives, and ensuring confidentiality. The code of ethics was obtained from Mazandaran University of Medical Sciences (IR.MAZUMS..REC.1399.403).
Funding
This project (No.: 7700) was carried out with the full support and funding of Mazandaran University of Medical Sciences and the Sexual Health and Fertility Research Center of Mazandaran University of Medical Sciences.
Authors' contributions
Conceptualization and Supervision: Erfaneh Talebi and Zohreh Shahhosseini; Methodology: Zohreh Shahhosseini and Soheila Rabiepoor; Data collection: Erfaneh Talebi and Zohreh Shahhosseini; Data analysis: Zohreh Shahhosseini and Monirolsadate Hosseini-Tabaghdehi; Funding acquisition and Resources: Erfaneh Talebi and Zohreh Shahhosseini. Investigation, Writing–original draft, and Writing-review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We express our gratitude to Mazandaran University of Medical Sciences for the financial support of this project (project number 7700) and all the participants who helped us conduct the research.
References
- Panahi R, Kheiri M, Daronkolaei ZA, Arjeini Z, Taherpour M, Dehghankar L, et al. The effect of sexual health literacy on the sexual life quality of women referring to healthcare centers in Qazvin, Iran. J Educ Health Promot. 2021; 10:1-8. [DOI:10.4103/jehp.jehp_1484_20] [PMID] [PMCID]
- Nash SD, Cruickshanks KJ, Klein R, Klein BE, Nieto FJ, Huang GH, et al. The prevalence of hearing impairment and associated risk factors: The Beaver Dam offspring study. Arch Otolaryngol Head Neck Surg. 2011; 137(5):432-9. [DOI:10.1001/archoto.2011.15] [PMID] [PMCID]
- Parvandi A, Arefi M, Moradi A. [The role of family functioning and couples communication patterns in marital satisfaction (Persian)]. Fam Pathol Couns Enrichment J. 2016; 2(1):54-65. [Link]
- Gilbert P. Compassion: Conceptualisations, research and use in psychotherapy. Abingdon: Routledge; 2004. [Link]
- Nejat S. [Quality of life and its measurement (Persian)]. Iran J Epidemiol. 2008; 4(2):57-62. [Link]
- Lamyian M, Zarei F, Montazeri A, Hajizadeh E, Maasoumi R. [Exploring the factors affecting Iranian women’s quality of sexual life (Persian)]. Hayat. 2016; 22(2):185-200. [Link]
- Stephenson KR, Meston CM. Differentiating components of sexual well-being in women: Are sexual satisfaction and sexual distress independent constructs? J Sex Med. 2010; 7(7):2458-68. [DOI:10.1111/j.1743-6109.2010.01836.x] [PMID]
- Dogan T, Tugut N, Golbasi Z. The relationship between sexual quality of life, happiness, and satisfaction with life in married Turkish women. Sex Disabil . 2013; 31:239-47. [DOI:10.1007/s11195-013-9302-z]
- Roshan Chesli R, Soleimani Z, Erfan T, Mantashlou S, Hashemi A. [Evaluate the psychometric properties of sexual quality of life questionnaire (SQOL-F) (Persian)]. Clin Psychol. 2020; 17(1):213-24. [DOI:10.22070/CPAP.2020.2898]
- Ayles C. Biographical determinates of marital quality. London: One Plus One; 2004. [Link]
- Fincham FD, Beach SR. Marriage in the new millennium: A decade in review. J Marriage Fam. 2010; 72(3):630-49. [DOI:10.1111/j.1741-3737.2010.00722.x]
- Hisli Şahin N, Durak Batıgün A, Alkan Pazvantoğlu E. [The role of interpersonal style, self perception and anger in sexual dysfunction (Turkish)]. Turk Psikiyatri Derg. 2012; 23(1):18-25. [PMID]
- Holmberg D, Blair KL, Phillips M. Women’s sexual satisfaction as a predictor of well-being in same-sex versus mixed-sex relationships. J Sex Res. 2010; 47(1):1-11. [DOI:10.1080/00224490902898710] [PMID]
- Kwadwo W, Anafi P, Sekyere FO. Does disability matter? Disability in sexual and reproductive health policies and research in Ghana. Community Health Equity Research & Policy. 2014; 35(1):21-35. [DOI:10.2190/IQ.35.1.c]
- World Health Organization. Promoting sexual and reproductive health for persons with disabilities: WHO/UNFPA guidance note.Geneva: World Health Organization; 2009.[Link]
- Groce NE. Adolescents and youth with disability: Issues and challenges. Asia Pac Disabil Rehabil J. 2004; 15(2):13-32. [Link]
- Symonds T, Boolell M, Quirk F. Development of a questionnaire on sexual quality of life in women. J Sex Marital Ther. 2005; 31(5):385-97. [DOI:10.1080/00926230591006502] [PMID]
- Maasoumi R, Lamyian M, Montazeri A, Azin SA, Aguilar-Vafaie ME, Hajizadeh E. The sexual quality of life-female (SQOL-F) questionnaire: Translation and psychometric properties of the Iranian version. Reprod Health. 2013; 10:25. [DOI:10.1186/1742-4755-10-25] [PMID] [PMCID]
- Kuenburg A, Fellinger P, Fellinger J. Health care access among deaf people. J Deaf Stud Deaf Educ. 2016; 21(1):1-10. [DOI:10.1093/deafed/env042] [PMID]
- Tsimpida D, Kaitelidou D, Galanis P. Determinants of health-related quality of life (HRQoL) among deaf and hard of hearing adults in Greece: A cross-sectional study. Arch Public Health. 2018; 76:65. [DOI:10.1186/s13690-018-0304-2] [PMID] [PMCID]
- Ganle JK, Baatiema L, Quansah R, Danso-Appiah A. Barriers facing persons with disability in accessing sexual and reproductive health services in sub-Saharan Africa: A systematic review. Plos One. 2020; 15(10):e0238585. [DOI:10.1371/journal.pone.0238585] [PMID] [PMCID]
Type of Study: Research |
Subject:
Family health
Received: 2022/10/11 | Accepted: 2022/12/20 | Published: 2022/10/1
Received: 2022/10/11 | Accepted: 2022/12/20 | Published: 2022/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
