Wed, May 27, 2026
[Archive]
Volume 3, Issue 1 (Autumn 2024)
CPR 2024, 3(1): 25-32 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadeghi A, Raissi-Dehkordi N, Eliaei S, Rastegar R, Cheraghpour M, Hatami H et al . Prevalence of Anxiety and Depression Among Patients With Symptomatic Choledocholithiasis: A Cross-sectional Study in Iran. CPR 2024; 3 (1) :25-32
URL: http://cpr.mazums.ac.ir/article-1-153-en.html
URL: http://cpr.mazums.ac.ir/article-1-153-en.html
Amir Sadeghi 

 , Nastaran Raissi-Dehkordi , Shiva Eliaei , Reyhaneh Rastegar , Makan Cheraghpour , Hossein Hatami , Negar Raissi Dehkordi
, Nastaran Raissi-Dehkordi , Shiva Eliaei , Reyhaneh Rastegar , Makan Cheraghpour , Hossein Hatami , Negar Raissi Dehkordi
, Nastaran Raissi-Dehkordi , Shiva Eliaei , Reyhaneh Rastegar , Makan Cheraghpour , Hossein Hatami , Negar Raissi Dehkordi
Department of Public Health, Safety and Environmental and Occupational Hazards Control Research Center, School of Public Health, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Keywords: Gallbladder diseases, Choledocholithiasis, Anxiety disorders, Depressive disorder, Mental disorders
Full-Text [PDF 614 kb]
(36 Downloads)
| Abstract (HTML) (109 Views)
Full-Text: (19 Views)
Introduction
Diseases of the gallbladder constitute a major health concern, affecting more than 52 million adults worldwide [1]. Among these conditions, symptomatic choledocholithiasis, characterized by the presence of obstructive gallstones within the common bile duct (CBD), poses a significant clinical challenge [2]. Timely diagnosis and management of choledocholithiasis are crucial, as untreated cases may lead to severe complications such as cholangitis and pancreatitis [3].
In Iran, a country with a notable prevalence of gallbladder disorders, understanding the multifaceted factors influencing choledocholithiasis becomes paramount [4]. Beyond the physical aspects of this condition, there exists a growing body of evidence indicating potential links between mental health disorders, specifically anxiety and depression, and gastrointestinal ailments [5].
Depression and anxiety are among the major causes of disability worldwide [6]. Globally, depression affects about 3.8% of the population (5% among adults), and anxiety disorders affect approximately 4%, corresponding to more than 300 million people worldwide [7]. Anxiety and depression are common psychiatric symptoms among patients with chronic disease [8]. Studies show that patients with gallstones face a higher risk for developing depression compared to the general population [9, 10]. Chronic pain or inflammation might be the underlying mechanisms for development of depression in patients with cholelithiasis, however the exact underlying mechanisms are not known [11].
Identifying the link between depression, anxiety, and choledocholithiasis is necessary for effective prevention and treatment of the disease. When psychological symptoms coincide with choledocholithiasis, they can worsen the condition, leading to poorer outcomes and delayed management, thereby diminishing patients’ overall quality of life. Previous research has shown that individuals with gallstone disease experience a higher prevalence of depressive symptoms compared with the general population, and that inflammation and chronic pain may play a role in this association, emphasizing the importance of early psychological screening to reduce the impact of depression and anxiety on disease progression and patient wellbeing [9, 10].
Despite known links between gallstones and psychiatric symptoms, data on anxiety and depression specifically in symptomatic CBD stones, especially in Iranian populations, are limited. Therefore, we conducted a cross-sectional study to determine the prevalence of anxiety and depression and their associations with clinical and demographic factors in this group.
Methods and Materials
Patients and study design
This cross-sectional study was conducted at Taleghani Teaching Hospital in Tehran, Iran, between June 2023 and August 2023. The study included patients undergoing Endoscopic Retrograde Cholangiopancreatography (ERCP) for the treatment of symptomatic CBD stones. Participants were selected using a consecutive sampling method, meaning all eligible patients presenting during the study period were invited to participate. A total of 265 patients were screened, and 215 who met the inclusion criteria and provided written informed consent were included in the analysis. The eligibility criteria for recruitment were as follows: (1) Age >8, (2) clinical diagnosis of CBD stone, (3) no history of treatment for CBD stone, and (4) Absence of cognitive impairment and ability to participate in the hospital anxiety and depression scale (HADS) questionnaire. Exclusion criteria were (1) diagnosis of a gastrointestinal disorder other than CBD stone, (2) having a diagnosis of previous psychological disorder, (3) active pregnancy or lactation, (4) severe cardiovascular disease, (5) participants with an unreasonable body mass index (BMI) (<15 or >50 kg/m²), and (5) those with missing or incomplete dietary or general lifestyle information.
Evaluation of CBD stone
The criteria for clinical diagnosis included evidence of CBD dilation in ultrasonography followed by evidence of CBD stone in ERCP. All endoscopic examinations were performed by board-certified gastroenterologists. Conventional white light endoscopes were used for all procedures.
Assessment of depression and anxiety
Anxiety and depression were assessed using the HADS, which consists of 14 items—7 for anxiety (HADS-A) and 7 for depression (HADS-D) [12]. Each item is scored from 0 to 3, giving a total score range of 0–21 for each subscale. A score of 0–7 indicates normal, 8–10 borderline, and 11–21 abnormal levels of anxiety or depression. The Iranian version of HADS has been previously validated in Iranian populations, showing high internal consistency (Cronbach’s α=0.78 for HADS-A and 0.86 for HADS-D) and construct validity [13].
Clinical and laboratory evaluations
The primary outcome variables were HADS-A and HADS-D scores. Demographic/lifestyle characteristics were collected via questionnaire and are presented in Table 1. Associations between HADS scores and continuous variables (weight, height, BMI, serum amylase, and stone size) were evaluated using simple linear regression. Data regarding medical history, demographic, lifestyle, and psychosocial background of patients was obtained from a self-administered questionnaire. A digital scale was used to measure height and body weight. Laboratory tests were performed on the day of admission.
Statistical analysis
Data were analyzed using IBM SPSS software, version 24.0 (IBM Corp., Armonk, NY, USA). The normality of quantitative variables was evaluated using the Kolmogorov–Smirnov test. Variables that were normally distributed are presented as Mean±SD and were analyzed using the Student’s t-test; non-normally distributed variables are reported as median (interquartile range) and were analyzed using the Mann–Whitney U test. Categorical variables were compared using the chi-square test.
To explore the relationship between HADS scores and continuous demographic or clinical variables, simple linear regression analyses were performed. Before interpreting the regression results, the assumptions of linearity, independence of errors, homoscedasticity, and normal distribution of residuals were examined. Linearity was verified by scatterplots of predictors versus HADS scores, independence of errors by the Durbin–Watson statistic, homoscedasticity by plotting standardized residuals versus predicted values, and normality of residuals by inspecting P–P plots. All tests were two-tailed, and a P<0.05 was considered statistically significant. Missing data were minimal; analyses were based on the available observed data for each variable, and no imputation procedures were applied.
Results
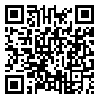
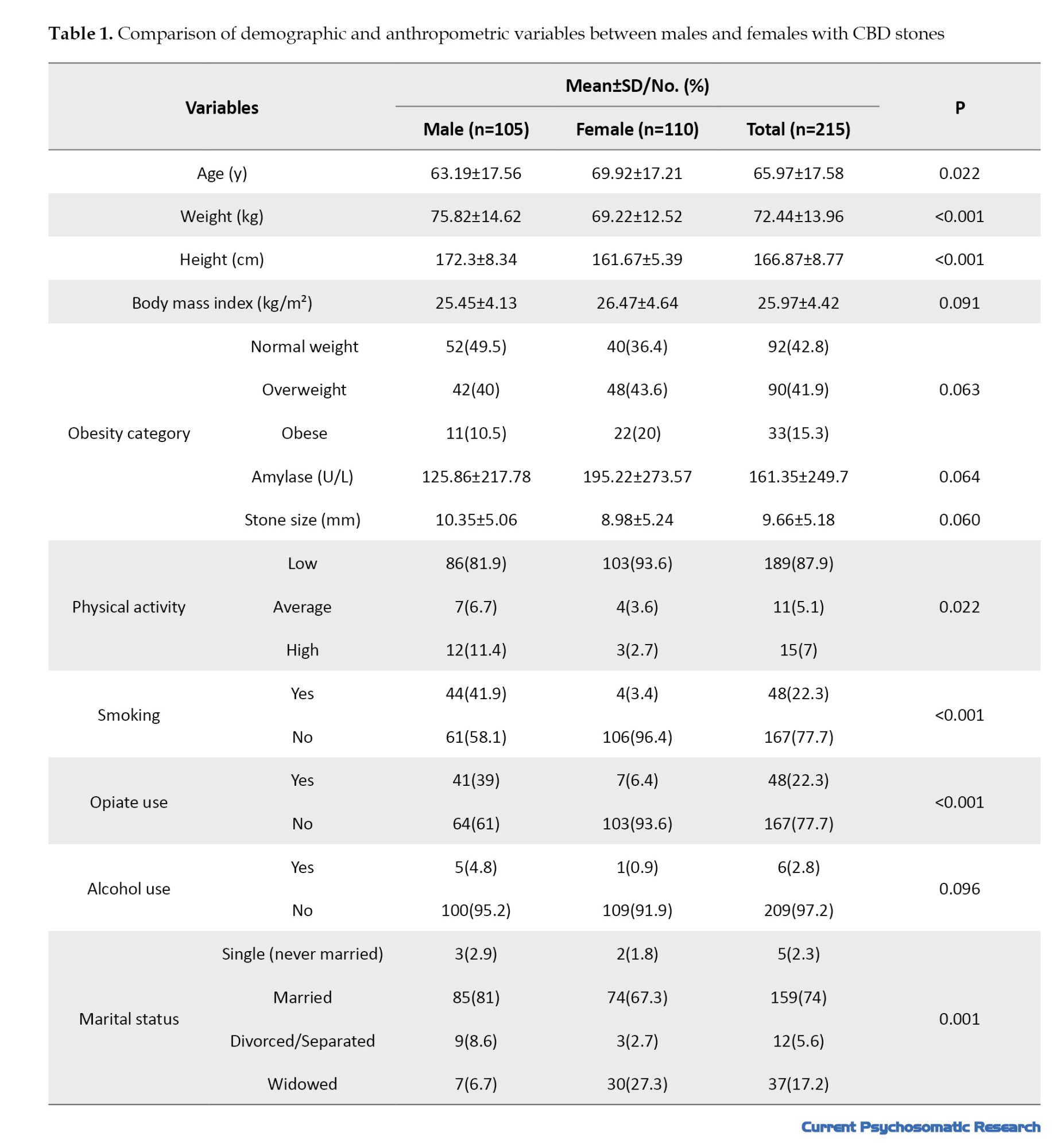
Table 1 provides an overview of the patient characteristics. The participants in this study had a mean age of 65.9±11.9 years. The distribution of genders was 51.2% women and 48.8% men. The prevalence of anxiety and depression stood at 39.5% and 24.2%, respectively. The proportions of males and females in each HADS anxiety category and in each HADS depression category were broadly similar (Table 2).
The comparison of demographic and anthropometric characteristics between male and female patients with CBD stones is presented in Table 1. Female patients were significantly older than males (69.9±17.2 vs 63.2±17.6 years, P=0.022) and had lower body weight and height (P<0.001). There was no significant difference in BMI (P=0.091), although obesity tended to be more common in females (20.%) than males (10.5%). Physical activity was generally lower among females (P=0.022). Smoking and opiate use were markedly higher in males (P<0.001), whereas alcohol use was uncommon in both sexes. Marital status also differed significantly between genders (P=0.001).
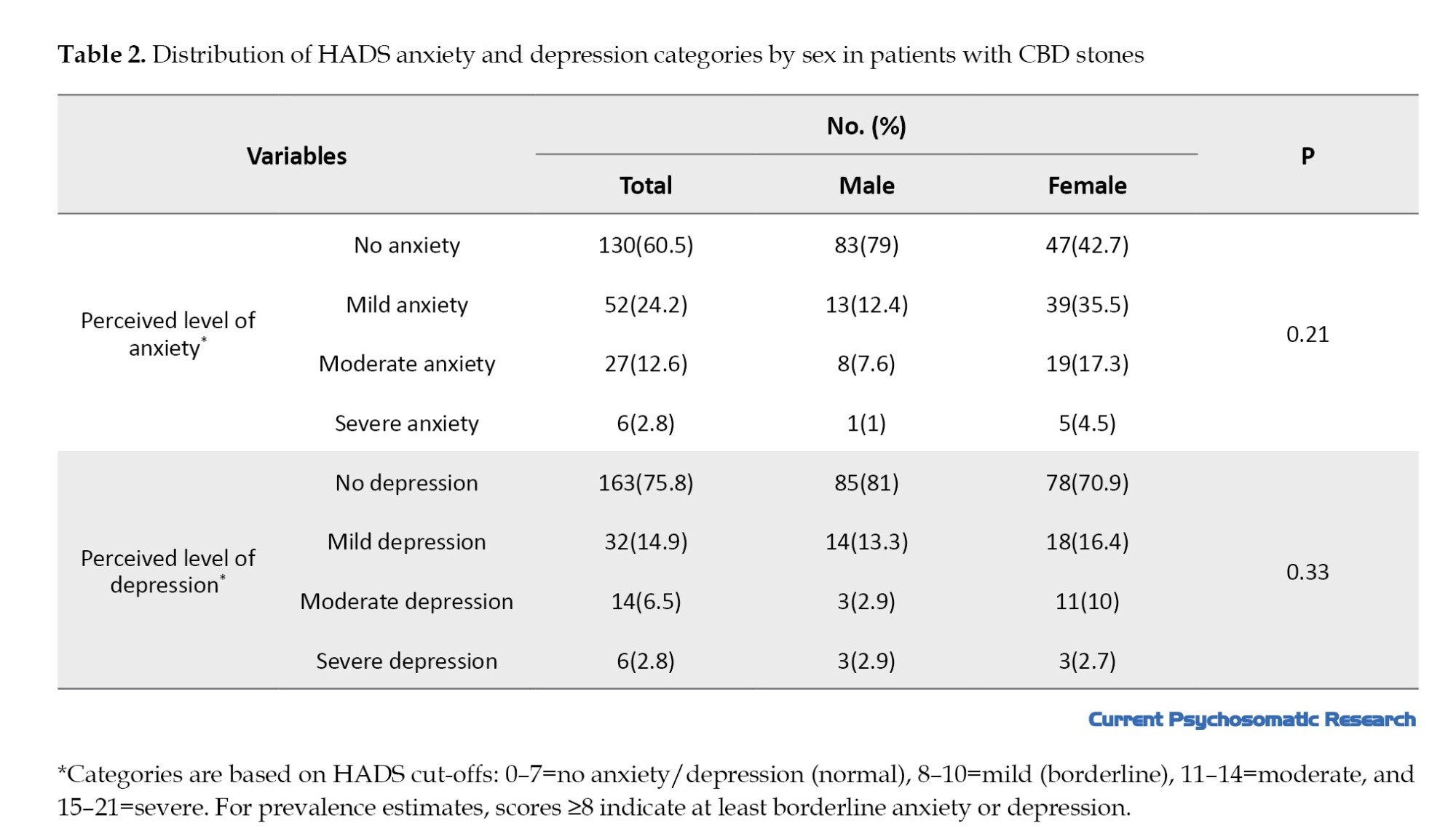
In simple linear regression, none of the demographic or anthropometric variables—weight, height, BMI, amylase, or stone size—were associated with HADS score in the overall cohort or within sex strata (all P>0.05); in the overall model, some trends including amylase (B≈0.003, P=0.066) and height (B≈−0.084, P=0.080) approached significance, but did not reach conventional statistical significance; these P values are reported as trends only and are not interpreted as significant findings. BMI, weight, and stone size were null (e.g. stone size B≈0, P≈0.999) (Table 3).
Discussion
Our study measured the prevalence of anxiety and depression at 39.5% and 24.2%, respectively. To the best of our knowledge, the relationship between anxiety and depression with prevalence of CBD stones has not been previously reported in Iran. Studies in other countries have reported similar results. A 2024 Mendelian randomization study on 1706 cases of bile duct stones and 461304 controls found that depression may increase the risk of cholelithiasis [14]. Prevalence of anxiety was reported to be 25% in patients with gallbladder stone and 36.0% in post-cholecystectomy patients [15]. These findings are in line with the results reported in the present study.
In this study, anxiety and depression were present in 39.5% and 24.2% of patients with symptomatic CBD stones, respectively. The prevalence of psychiatric disorders in Iran is reported to be 31.03% (95% CI, 25.995%, 36.07%) [16]. A recent study estimated the prevalence of depression in Iran to range from 5.69% to 73% [17], and the 12-month prevalence of anxiety disorders was reported to be 15.6% in a 2018 study of major anxiety disorders in Iran [18]. A systematic review of Iranian patients found the prevalence of depression to be 34.26% (95% CI, 24.12%, 44.1%) [19]. Another systematic review offered a more conservative estimate of depression prevalence in the general population at 19.46% [20]. The prevalence of anxiety and depression was higher in our study group compared to previous reports in the general population in Iran, pointing to a possible association between anxiety and depression with CBD stone occurrence. The observed differences in prevalence of anxiety and depression in our study with previous studies may be explained, in part, with the method of measuring these diseases. A systematic review and meta-analysis of 145 articles on the prevalence of depression in Iran found that 15 different tools were used to measure depression, mainly standard tools such as Beck’s and general health questionnaires [21]. Estimates of disease prevalence were dependent on the type of tests used; Beck’s inventory pointed to a depression rate of 37.22% in the general population, while general health questionnaires indicated a prevalence of 19.46%. It is plausible that the results would differ when using another questionnaire, as is the case in this study. The association between gastrointestinal diseases and depression has received significant attention, although the precise underlying mechanisms remain elusive. Inflammation emerges as a pivotal factor in this relationship. Elevated levels of cytokines and inflammatory markers such as TNF-a, IL-6, and IL-1β have been observed in individuals diagnosed with depression [22]. Notably, this inflammatory process shows signs of reversal upon the administration of antidepressant agents, suggesting a potential modulatory role of these agents in mitigating inflammation-associated depressive symptoms.
Anxiety and depression may also aggravate somatic and biliary symptoms. Inflammatory mediators and the gut–brain axis provide bidirectional links between gastrointestinal pathology and mood, potentially creating a cycle in which biliary disease and psychological distress perpetuate one another.
Furthermore, chronic pain has been identified as a contributory factor, potentially intensifying rates of anxiety and depression in patients grappling with chronic disease. This association underscores the importance of recognizing and addressing pain as a potential precipitant of mental health challenges, particularly in the context of gastrointestinal ailments [23].
Prompt diagnosis and treatment of depression and anxiety holds promise in improving the overall quality of life (QoL) for individuals contending with choledocholithiasis. Early intervention in mental health concerns may enable a more favorable response to therapeutic interventions. This dual approach, targeting both the physical manifestations of choledocholithiasis and the associated mental health dimensions, may contribute to improved patient outcomes and well-being [24].
Although several studies have demonstrated higher rates of anxiety and depression among patients with gallstone or biliary disease, other investigations have reported conflicting results. For example, Pan et al. (2024) [25] found no significant association between gallstones and depressive symptoms in a large U.S. adult population, while Tsai et al. (2015) [26] and Yu et al. (2025) [27] reported no long-term increase in depression risk after cholecystectomy. Such inconsistencies may stem from differences in study design, disease stage, follow-up duration, or population characteristics. Variation in psychometric tools, particularly the use of instruments other than the HADS, may also influence reported prevalence. Cultural factors and differences in pain perception or health-care access could further explain why psychological symptoms are more evident in some cohorts than others.
The present study did not identify significant associations between demographic and anthropometric parameters, including BMI, amylase level, stone size, and CBD stone.
When interpreting the results of this study, some limitations should be taken into account. Since the symptoms of anxiety and depression were recorded based on a self-reported questionnaire, there is a chance for underreporting or over-reporting of symptoms and recall bias. In addition, the observational nature of the study and the cross-sectional method means a causal inference cannot be derived from the observed results. Furthermore, our regression analyses were exploratory, and we modelled HADS-anxiety and HADS-depression scores as continuous outcomes in simple linear regression; although this is a commonly used approach, it may not fully capture the ordinal structure of the scales, and the resulting estimates should be regarded as hypothesis-generating. While the current study is helpful with regards to understanding the presence of anxiety and depression in patients with CBD stones, further research is warranted to dig deeper into the links between inflammation, pain, and mental health in the context of gastrointestinal diseases. By gaining a more complete understanding of the involved factors, healthcare providers can refine their treatment strategies, potentially affording patients a higher QoL and more effective therapeutic responses.
Conclusion
In conclusion, our study offered an estimate of the prevalence of anxiety and depression in the presence of CBD stones which is in concordance with previous reports. It is imperative to recognize that mental health is an important part of the clinical care of hospitalized patients, and our study may help improve the treatment and care offered to patients with CBD stones.
The findings indicate that anxiety and depression are common in patients with symptomatic choledocholithiasis and occur independently of measurable clinical or demographic factors. This suggests that psychological distress may be an intrinsic component of the illness experience rather than a secondary effect of disease severity. Clinically, incorporating routine mental health assessment—even brief tools like the HADS—could help identify at-risk patients early, improving communication, adherence, and overall care outcomes. Future studies should adopt prospective, multicenter designs with larger cohorts to determine causal relationships and evaluate whether targeted psychological interventions can improve both emotional wellbeing and recovery trajectories in this patient population.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Code: IR.SBMU.PHNS.REC.1402.024). The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All participants were informed about the study’s objectives, and written informed consent was obtained from each subject before enrollment.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
Diseases of the gallbladder constitute a major health concern, affecting more than 52 million adults worldwide [1]. Among these conditions, symptomatic choledocholithiasis, characterized by the presence of obstructive gallstones within the common bile duct (CBD), poses a significant clinical challenge [2]. Timely diagnosis and management of choledocholithiasis are crucial, as untreated cases may lead to severe complications such as cholangitis and pancreatitis [3].
In Iran, a country with a notable prevalence of gallbladder disorders, understanding the multifaceted factors influencing choledocholithiasis becomes paramount [4]. Beyond the physical aspects of this condition, there exists a growing body of evidence indicating potential links between mental health disorders, specifically anxiety and depression, and gastrointestinal ailments [5].
Depression and anxiety are among the major causes of disability worldwide [6]. Globally, depression affects about 3.8% of the population (5% among adults), and anxiety disorders affect approximately 4%, corresponding to more than 300 million people worldwide [7]. Anxiety and depression are common psychiatric symptoms among patients with chronic disease [8]. Studies show that patients with gallstones face a higher risk for developing depression compared to the general population [9, 10]. Chronic pain or inflammation might be the underlying mechanisms for development of depression in patients with cholelithiasis, however the exact underlying mechanisms are not known [11].
Identifying the link between depression, anxiety, and choledocholithiasis is necessary for effective prevention and treatment of the disease. When psychological symptoms coincide with choledocholithiasis, they can worsen the condition, leading to poorer outcomes and delayed management, thereby diminishing patients’ overall quality of life. Previous research has shown that individuals with gallstone disease experience a higher prevalence of depressive symptoms compared with the general population, and that inflammation and chronic pain may play a role in this association, emphasizing the importance of early psychological screening to reduce the impact of depression and anxiety on disease progression and patient wellbeing [9, 10].
Despite known links between gallstones and psychiatric symptoms, data on anxiety and depression specifically in symptomatic CBD stones, especially in Iranian populations, are limited. Therefore, we conducted a cross-sectional study to determine the prevalence of anxiety and depression and their associations with clinical and demographic factors in this group.
Methods and Materials
Patients and study design
This cross-sectional study was conducted at Taleghani Teaching Hospital in Tehran, Iran, between June 2023 and August 2023. The study included patients undergoing Endoscopic Retrograde Cholangiopancreatography (ERCP) for the treatment of symptomatic CBD stones. Participants were selected using a consecutive sampling method, meaning all eligible patients presenting during the study period were invited to participate. A total of 265 patients were screened, and 215 who met the inclusion criteria and provided written informed consent were included in the analysis. The eligibility criteria for recruitment were as follows: (1) Age >8, (2) clinical diagnosis of CBD stone, (3) no history of treatment for CBD stone, and (4) Absence of cognitive impairment and ability to participate in the hospital anxiety and depression scale (HADS) questionnaire. Exclusion criteria were (1) diagnosis of a gastrointestinal disorder other than CBD stone, (2) having a diagnosis of previous psychological disorder, (3) active pregnancy or lactation, (4) severe cardiovascular disease, (5) participants with an unreasonable body mass index (BMI) (<15 or >50 kg/m²), and (5) those with missing or incomplete dietary or general lifestyle information.
Evaluation of CBD stone
The criteria for clinical diagnosis included evidence of CBD dilation in ultrasonography followed by evidence of CBD stone in ERCP. All endoscopic examinations were performed by board-certified gastroenterologists. Conventional white light endoscopes were used for all procedures.
Assessment of depression and anxiety
Anxiety and depression were assessed using the HADS, which consists of 14 items—7 for anxiety (HADS-A) and 7 for depression (HADS-D) [12]. Each item is scored from 0 to 3, giving a total score range of 0–21 for each subscale. A score of 0–7 indicates normal, 8–10 borderline, and 11–21 abnormal levels of anxiety or depression. The Iranian version of HADS has been previously validated in Iranian populations, showing high internal consistency (Cronbach’s α=0.78 for HADS-A and 0.86 for HADS-D) and construct validity [13].
Clinical and laboratory evaluations
The primary outcome variables were HADS-A and HADS-D scores. Demographic/lifestyle characteristics were collected via questionnaire and are presented in Table 1. Associations between HADS scores and continuous variables (weight, height, BMI, serum amylase, and stone size) were evaluated using simple linear regression. Data regarding medical history, demographic, lifestyle, and psychosocial background of patients was obtained from a self-administered questionnaire. A digital scale was used to measure height and body weight. Laboratory tests were performed on the day of admission.
Statistical analysis
Data were analyzed using IBM SPSS software, version 24.0 (IBM Corp., Armonk, NY, USA). The normality of quantitative variables was evaluated using the Kolmogorov–Smirnov test. Variables that were normally distributed are presented as Mean±SD and were analyzed using the Student’s t-test; non-normally distributed variables are reported as median (interquartile range) and were analyzed using the Mann–Whitney U test. Categorical variables were compared using the chi-square test.
To explore the relationship between HADS scores and continuous demographic or clinical variables, simple linear regression analyses were performed. Before interpreting the regression results, the assumptions of linearity, independence of errors, homoscedasticity, and normal distribution of residuals were examined. Linearity was verified by scatterplots of predictors versus HADS scores, independence of errors by the Durbin–Watson statistic, homoscedasticity by plotting standardized residuals versus predicted values, and normality of residuals by inspecting P–P plots. All tests were two-tailed, and a P<0.05 was considered statistically significant. Missing data were minimal; analyses were based on the available observed data for each variable, and no imputation procedures were applied.
Results
Table 1 provides an overview of the patient characteristics. The participants in this study had a mean age of 65.9±11.9 years. The distribution of genders was 51.2% women and 48.8% men. The prevalence of anxiety and depression stood at 39.5% and 24.2%, respectively. The proportions of males and females in each HADS anxiety category and in each HADS depression category were broadly similar (Table 2).
The comparison of demographic and anthropometric characteristics between male and female patients with CBD stones is presented in Table 1. Female patients were significantly older than males (69.9±17.2 vs 63.2±17.6 years, P=0.022) and had lower body weight and height (P<0.001). There was no significant difference in BMI (P=0.091), although obesity tended to be more common in females (20.%) than males (10.5%). Physical activity was generally lower among females (P=0.022). Smoking and opiate use were markedly higher in males (P<0.001), whereas alcohol use was uncommon in both sexes. Marital status also differed significantly between genders (P=0.001).
In simple linear regression, none of the demographic or anthropometric variables—weight, height, BMI, amylase, or stone size—were associated with HADS score in the overall cohort or within sex strata (all P>0.05); in the overall model, some trends including amylase (B≈0.003, P=0.066) and height (B≈−0.084, P=0.080) approached significance, but did not reach conventional statistical significance; these P values are reported as trends only and are not interpreted as significant findings. BMI, weight, and stone size were null (e.g. stone size B≈0, P≈0.999) (Table 3).
Discussion
Our study measured the prevalence of anxiety and depression at 39.5% and 24.2%, respectively. To the best of our knowledge, the relationship between anxiety and depression with prevalence of CBD stones has not been previously reported in Iran. Studies in other countries have reported similar results. A 2024 Mendelian randomization study on 1706 cases of bile duct stones and 461304 controls found that depression may increase the risk of cholelithiasis [14]. Prevalence of anxiety was reported to be 25% in patients with gallbladder stone and 36.0% in post-cholecystectomy patients [15]. These findings are in line with the results reported in the present study.
In this study, anxiety and depression were present in 39.5% and 24.2% of patients with symptomatic CBD stones, respectively. The prevalence of psychiatric disorders in Iran is reported to be 31.03% (95% CI, 25.995%, 36.07%) [16]. A recent study estimated the prevalence of depression in Iran to range from 5.69% to 73% [17], and the 12-month prevalence of anxiety disorders was reported to be 15.6% in a 2018 study of major anxiety disorders in Iran [18]. A systematic review of Iranian patients found the prevalence of depression to be 34.26% (95% CI, 24.12%, 44.1%) [19]. Another systematic review offered a more conservative estimate of depression prevalence in the general population at 19.46% [20]. The prevalence of anxiety and depression was higher in our study group compared to previous reports in the general population in Iran, pointing to a possible association between anxiety and depression with CBD stone occurrence. The observed differences in prevalence of anxiety and depression in our study with previous studies may be explained, in part, with the method of measuring these diseases. A systematic review and meta-analysis of 145 articles on the prevalence of depression in Iran found that 15 different tools were used to measure depression, mainly standard tools such as Beck’s and general health questionnaires [21]. Estimates of disease prevalence were dependent on the type of tests used; Beck’s inventory pointed to a depression rate of 37.22% in the general population, while general health questionnaires indicated a prevalence of 19.46%. It is plausible that the results would differ when using another questionnaire, as is the case in this study. The association between gastrointestinal diseases and depression has received significant attention, although the precise underlying mechanisms remain elusive. Inflammation emerges as a pivotal factor in this relationship. Elevated levels of cytokines and inflammatory markers such as TNF-a, IL-6, and IL-1β have been observed in individuals diagnosed with depression [22]. Notably, this inflammatory process shows signs of reversal upon the administration of antidepressant agents, suggesting a potential modulatory role of these agents in mitigating inflammation-associated depressive symptoms.
Anxiety and depression may also aggravate somatic and biliary symptoms. Inflammatory mediators and the gut–brain axis provide bidirectional links between gastrointestinal pathology and mood, potentially creating a cycle in which biliary disease and psychological distress perpetuate one another.
Furthermore, chronic pain has been identified as a contributory factor, potentially intensifying rates of anxiety and depression in patients grappling with chronic disease. This association underscores the importance of recognizing and addressing pain as a potential precipitant of mental health challenges, particularly in the context of gastrointestinal ailments [23].
Prompt diagnosis and treatment of depression and anxiety holds promise in improving the overall quality of life (QoL) for individuals contending with choledocholithiasis. Early intervention in mental health concerns may enable a more favorable response to therapeutic interventions. This dual approach, targeting both the physical manifestations of choledocholithiasis and the associated mental health dimensions, may contribute to improved patient outcomes and well-being [24].
Although several studies have demonstrated higher rates of anxiety and depression among patients with gallstone or biliary disease, other investigations have reported conflicting results. For example, Pan et al. (2024) [25] found no significant association between gallstones and depressive symptoms in a large U.S. adult population, while Tsai et al. (2015) [26] and Yu et al. (2025) [27] reported no long-term increase in depression risk after cholecystectomy. Such inconsistencies may stem from differences in study design, disease stage, follow-up duration, or population characteristics. Variation in psychometric tools, particularly the use of instruments other than the HADS, may also influence reported prevalence. Cultural factors and differences in pain perception or health-care access could further explain why psychological symptoms are more evident in some cohorts than others.
The present study did not identify significant associations between demographic and anthropometric parameters, including BMI, amylase level, stone size, and CBD stone.
When interpreting the results of this study, some limitations should be taken into account. Since the symptoms of anxiety and depression were recorded based on a self-reported questionnaire, there is a chance for underreporting or over-reporting of symptoms and recall bias. In addition, the observational nature of the study and the cross-sectional method means a causal inference cannot be derived from the observed results. Furthermore, our regression analyses were exploratory, and we modelled HADS-anxiety and HADS-depression scores as continuous outcomes in simple linear regression; although this is a commonly used approach, it may not fully capture the ordinal structure of the scales, and the resulting estimates should be regarded as hypothesis-generating. While the current study is helpful with regards to understanding the presence of anxiety and depression in patients with CBD stones, further research is warranted to dig deeper into the links between inflammation, pain, and mental health in the context of gastrointestinal diseases. By gaining a more complete understanding of the involved factors, healthcare providers can refine their treatment strategies, potentially affording patients a higher QoL and more effective therapeutic responses.
Conclusion
In conclusion, our study offered an estimate of the prevalence of anxiety and depression in the presence of CBD stones which is in concordance with previous reports. It is imperative to recognize that mental health is an important part of the clinical care of hospitalized patients, and our study may help improve the treatment and care offered to patients with CBD stones.
The findings indicate that anxiety and depression are common in patients with symptomatic choledocholithiasis and occur independently of measurable clinical or demographic factors. This suggests that psychological distress may be an intrinsic component of the illness experience rather than a secondary effect of disease severity. Clinically, incorporating routine mental health assessment—even brief tools like the HADS—could help identify at-risk patients early, improving communication, adherence, and overall care outcomes. Future studies should adopt prospective, multicenter designs with larger cohorts to determine causal relationships and evaluate whether targeted psychological interventions can improve both emotional wellbeing and recovery trajectories in this patient population.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Code: IR.SBMU.PHNS.REC.1402.024). The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All participants were informed about the study’s objectives, and written informed consent was obtained from each subject before enrollment.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
- Liu S, Yi M, Qin J, Lei F, Lin L, Li Y, et al. The increasing incidence and high body mass index-related burden of gallbladder and biliary diseases-A results from global burden of disease study 2019. Front Med. 2022; 9:1002325. [DOI:10.3389/fmed.2022.1002325] [PMID]
- Molvar C, Glaenzer B. Choledocholithiasis: Evaluation, treatment, and outcomes. Semin Intervent Radiol. 2016; 33 (4):268-76. [DOI:10.1055/s-0036-1592329] [PMID]
- Maple JT, Ben-Menachem T, Anderson MA, Appalaneni V, Banerjee S, Cash BD, et al. The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointest Endosc. 2010; 71 (1):1-9. [DOI:10.1016/j.gie.2009.09.041] [PMID]
- Zamani F, Sohrabi M, Alipour A, Motamed N, Saeedian FS, Pirzad R, et al. Prevalence and risk factors of cholelithiasis in Amol city, northern Iran: A population based study. Arch Iran Med. 2014; 17 (11):750-4.
- Shah E, Rezaie A, Riddle M, Pimentel M. Psychological disorders in gastrointestinal disease: epiphenomenon, cause or consequence? Ann Gastroenterol Hepatol. 2014; 27(3):224-30.
- Friedrich MJ. Depression is the leading cause of disability around the world. JAMA. 2017; 317 (15):1517. [DOI:10.1001/jama.2017.3826]
- Evans-Lacko S, Aguilar-Gaxiola S, Al-Hamzawi A, Alonso J, Benjet C, Bruffaerts R, et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: Results from the WHO World Mental Health (WMH) surveys. Psychol Med. 2018; 48 (9):1560-71. [DOI:10.1017/S0033291717003336] [PMID]
- Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. Lancet. 2007; 370 (9590):851-8. [DOI:10.1016/S0140-6736 (07)61415-9] [PMID]
- Shen TC, Lai HC, Huang YJ, Lin CL, Sung FC, Kao CH. The risk of depression in patients with cholelithiasis before and after cholecystectomy: A population-based cohort study. Medicine. 2015; 94 (10):e631. [DOI:10.1097/MD.0000000000000631] [PMID]
- Ma R, Li W, Peng Q, Ren A, Zhao L, Li J, et al. Association between gallstones and depressive symptoms: Results from NHANES and Mendelian randomization study. Psychol Res Behav Manag. 2024; 17:3659-76. [DOI:10.2147/PRBM.S477449] [PMID]
- Sheng J, Liu S, Wang Y, Cui R, Zhang X. The link between Depression and Chronic Pain: Neural mechanisms in the brain. Neural Plast. 2017; 2017:9724371. [DOI:10.1155/2017/9724371] [PMID]
- Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. 2002; 52(2):69-77. [DOI:10.1016/S0022-3999 (01)00296-3] [PMID]
- Montazeri A, Vahdaninia M, Ebrahimi M, Jarvandi S. The hospital anxiety and depression scale (HADS): Translation and validation study of the Iranian version. Health Qual Life Outcomes. 2003; 1(1):14. [DOI:10.1186/1477-7525-1-14] [PMID]
- Kong Y, Yao Z, Ren L, Zhou L, Zhao J, Qian Y, et al. Depression and hepatobiliary diseases: a bidirectional Mendelian randomization study. Front Psychiatry. 2024; 15:1366509. [DOI:10.3389/fpsyt.2024.1366509] [PMID]
- Li X, Zhang W, Pan Z, Shen R. Cohort analysis of relevant factors for negative emotions during the perioperative period in choledocholithiasis patients treated with ERCP and the impact on prognosis. Gland Surg. 2023; 12(5):651-63. [DOI:10.21037/gs-23-150] [PMID]
- Taheri Mirghaed M, Abolghasem Gorji H, Panahi S. Prevalence of psychiatric disorders in Iran: A systematic review and meta-analysis. Int J Prev Med. 2020; 11(1):21. [DOI:10.4103/ijpvm.IJPVM_510_18] [PMID]
- Montazeri A, Mousavi SJ, Omidvari S, Tavousi M, Hashemi A, Rostami T. Depression in Iran: A systematic review of the literature (2000-2010). Payesh. 2013; 12(6):567-94.
- Hajebi A, Motevalian SA, Rahimi-Movaghar A, Sharifi V, Amin-Esmaeili M, Radgoodarzi R, et al. Major anxiety disorders in Iran: prevalence, sociodemographic correlates and service utilization. BMC Psychiatry. 2018; 18(1):261. [DOI:10.1186/s12888-018-1828-2] [PMID]
- Tahan M, Saleem T, Zygoulis P, Pires LVL, Pakdaman M, Taheri H, et al. A systematic review of prevalence of Depression in Iranian patients. Neuropsychopharmacol Hung. 2020; 22(1):16-22.
- Sarokhani D, Parvareh M, Hasanpour Dehkordi A, Sayehmiri K, Moghimbeigi A. Prevalence of depression among Iranian elderly: Systematic review and meta-analysis. Iran J Psychiatry. 2018; 13(1):55-64.
- Mohamadi M, Mohaqeqi Kamal SH, Vameghi M, Rafiey H, Setareh Forouzan A, Sajjadi H. A meta-analysis of studies related prevalence of depression in Iran. J Res Health Sci. 2017; 7(1):581-93. [DOI:10.18869/acadpub.jrh.7.1.581]
- Wang L, Wang R, Liu L, Qiao D, Baldwin DS, Hou R. Effects of SSRIs on peripheral inflammatory markers in patients with major depressive disorder: A systematic review and meta-analysis. Brain Behav Immun. 2019; 79:24-38. [DOI:10.1016/j.bbi.2019.02.021] [PMID]
- Woo AK. Depression and anxiety in pain. Rev Pain. 2010; 4(1):8-12. [DOI:10.1177/204946371000400103] [PMID]
- Choi JM, Chung GE, Kang SJ, Kwak MS, Yang JI, Park B, et al. Association between anxiety and depression and nonalcoholic fatty liver disease. Front Med. 2020; 7:585618. [DOI:10.3389/fmed.2020.585618] [PMID]
- Pan T, Zhang C, Liang J, Wang X, Di X, Zhou Y, et al. Association between life-ever gallstones and depressive symptoms in U.S. adults: A cross-sectional study. Sci Rep. 2024; 14(1):18845. [DOI:10.1038/s41598-024-69777-7] [PMID]
- Tsai MC, Chen CH, Lee HC, Lin HC, Lee CZ. Increased risk of depressive disorder following cholecystectomy for gallstones. Plos One. 2015; 10 (6):e0129962. [DOI:10.1371/journal.pone.0129962] [PMID]
- Yu J, Park S, Jeong S, Ko A, Lee J, Han S, et al. Association of cholecystectomy with short-term and long-term risks of depression and suicide. Sci Rep. 2025; 15 (1):6557. [DOI:10.1038/s41598-025-87523-5] [PMID]
Type of Study: Research |
Subject:
Psychology
Received: 2024/06/3 | Accepted: 2024/08/26 | Published: 2024/10/1
Received: 2024/06/3 | Accepted: 2024/08/26 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
