Wed, May 27, 2026
[Archive]
Volume 3, Issue 1 (Autumn 2024)
CPR 2024, 3(1): 5-14 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Karimi P, Samaei Jablou R, Khaledi A, Nakhli M. The Role of Childhood Trauma in the Development of Psychosomatic Symptoms in Adulthood: A Narrative Review. CPR 2024; 3 (1) :5-14
URL: http://cpr.mazums.ac.ir/article-1-150-en.html
URL: http://cpr.mazums.ac.ir/article-1-150-en.html



Department of Clinical Psychology, University of Science and Art, Yazd, Iran.
Full-Text [PDF 745 kb]
(38 Downloads)
| Abstract (HTML) (103 Views)
Full-Text: (22 Views)
Introduction
Asubstantial body of research in psychosomatic medicine demonstrates that various somatic conditions can emerge as direct consequences of psychological disturbances, highlighting the intricate mind-body interconnection [1]. Prolonged exposure to chronic stress, persistent anxiety, and unprocessed traumatic experiences can induce significant dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, subsequently triggering a cascade of pathophysiological alterations [2]. At the neurobiological level, this psychophysiological interplay is mediated through aberrant neurotransmitter signaling and dysfunction within the autonomic nervous system [3]. Empirical evidence further reveals that depressive disorders are associated with elevated levels of proinflammatory cytokines, which may potentiate cardiovascular pathology, whereas somatization disorders frequently present with medically unexplained physical symptoms in the absence of a detectable organic etiology. These findings collectively underscore the propensity for psychological distress to translate into somatic manifestations [4].
Psychosomatic symptoms represent a complex interplay between psychological distress and physiological manifestations, where emotional or cognitive factors directly contribute to physical dysfunction without clear organic pathology [4]. These symptoms often manifest as gastrointestinal disturbances (e.g. irritable bowel syndrome) or cardiovascular irregularities (e.g. hypertension), mediated by dysregulated stress responses via the HPA axis and autonomic nervous system overactivation [5]. Neuroimaging studies implicate altered activity in limbic regions (e.g. the amygdala and anterior cingulate cortex) that modulate pain perception and visceral sensitivity. Notably, conditions, such as conversion disorder, demonstrate symptom specificity (e.g. paralysis, pseudoseizures), reflecting subconscious psychological conflicts [6].
Psychosomatic symptoms can precipitate a cascade of debilitating physiological and psychological consequences, creating a vicious cycle of impairment [7]. Medically unexplained symptoms (e.g. chronic pain, fatigue, or gastrointestinal distress) often lead to repeated, fruitless medical investigations, fostering patient frustration and eroding trust in healthcare systems [8]. Psychologically, these symptoms correlate with heightened anxiety and depressive disorders due to persistent distress and perceived loss of bodily control. Cognitive distortions, such as catastrophic thinking or health-related hypervigilance, may develop, exacerbating symptom severity and functional disability [9]. Socially, individuals frequently experience stigmatization—dismissed as “fabricating” illness—which compounds isolation and reduces treatment adherence [10]. Over time, the chronicity of psychosomatic conditions can induce maladaptive coping strategies (e.g. avoidance behaviors), further entrenching mind-body dysfunction, and diminishing quality of life [11].
Given the aforementioned consequences, identifying the contributing factors to psychosomatic symptoms would be highly beneficial for preventive interventions. Childhood trauma can precipitate the development of psychosomatic symptoms through persistent maladaptive changes in neurobiological stress-response systems and emotional processing pathways [12]. Early adverse experiences (e.g. abuse, neglect) induce chronic hyperactivity of the HPA axis, leading to prolonged cortisol exposure that disrupts immune function and promotes systemic inflammation [13]. Concurrently, trauma alters limbic system connectivity (particularly amygdala hyperactivity and prefrontal cortex dysregulation), impairing affect modulation and amplifying interoceptive sensitivity to bodily sensations [13]. These neurophysiological adaptations manifest as heightened somatic awareness and dysfunctional autonomic nervous system responses, wherein psychological distress becomes somatized with chronic pain, gastrointestinal disturbances, or conversion symptoms [14]. Furthermore, trauma-related dissociation may fragment the cognitive processing of emotional distress, redirecting it through somatic channels [14]. Epigenetic modifications of stress-related genes and enduring attachment disruptions further entrench this mind-body dysregulation, creating a diathesis for psychosomatic disorders that often persist into adulthood [15].
This narrative review is critically needed to synthesize the growing yet disparate body of evidence linking childhood trauma to adult psychosomatic pathology, while addressing significant gaps in current understanding. This study’s innovation lies in its interdisciplinary approach—bridging developmental psychopathology and psychoneuroimmunology to propose a unified biopsychosocial model of trauma-induced somatization. It addresses explicitly under-researched areas, such as the dose-response relationship between trauma subtypes (emotional vs physical abuse) and specific somatic symptom clusters, as well as protective resilience factors.
Materials and Methods
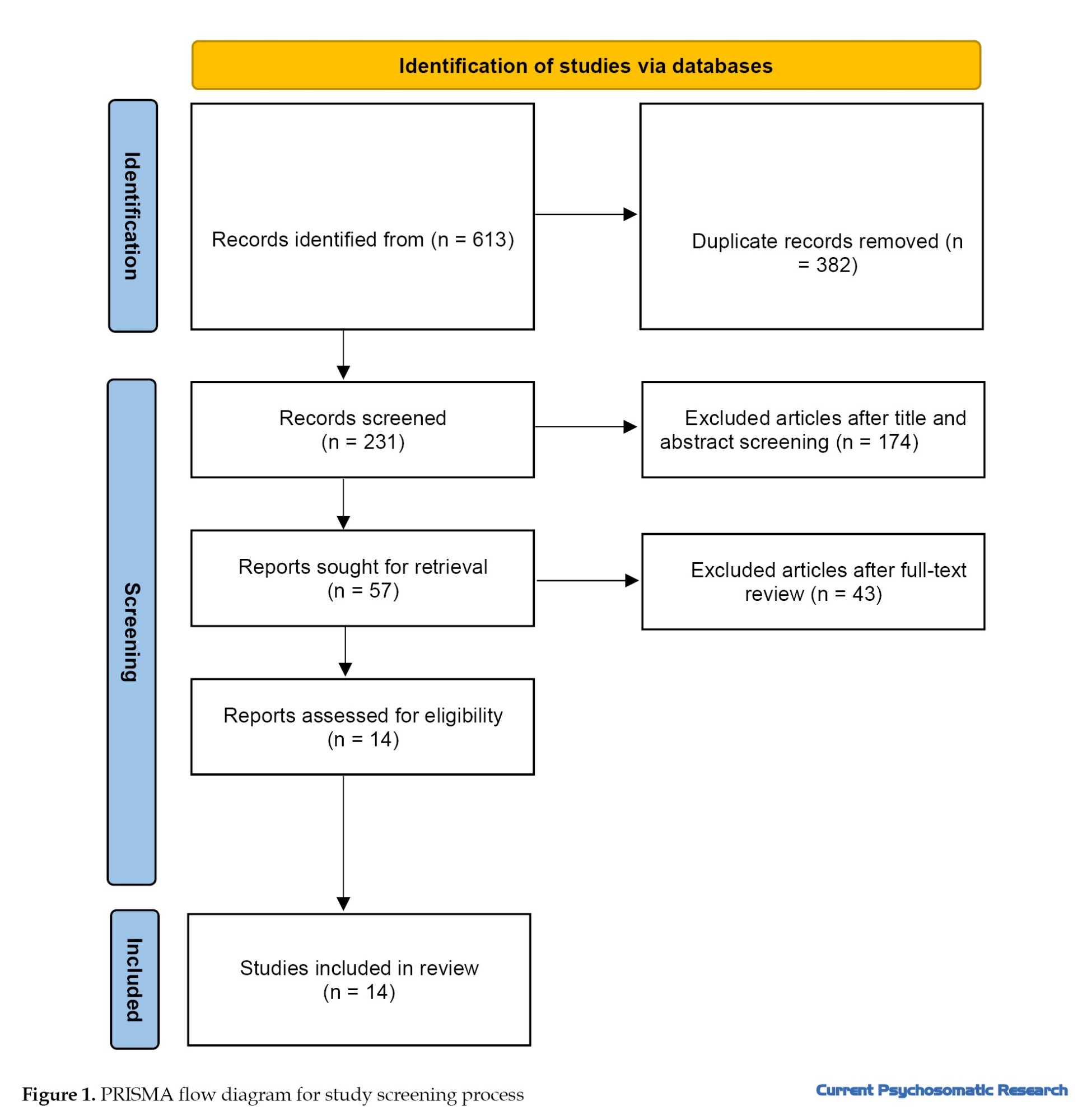
This study employed a narrative (non-systematic) review methodology, as this approach offers flexibility in synthesizing findings from studies with diverse designs and enables qualitative analysis. The inclusion criteria encompassed primary research investigating the role of childhood trauma in the development of psychosomatic symptoms in adulthood. Accordingly, all eligible cross-sectional, cohort, and other relevant studies were included. A comprehensive search was conducted across four international databases (Web of Science, PubMed, Scopus, and Google Scholar) for publications from 2016 to 2025. Additionally, the reference lists of all selected review articles identified in the initial screening phase were thoroughly examined to ensure comprehensive coverage of relevant literature (Figure1).
The search was conducted using combined keywords of “childhood trauma” OR “childhood trauma” OR “child maltreatment” OR “child abuse” OR “childhood adversity” OR “adverse childhood experiences” OR “emotional abuse” OR “psychological abuse” OR “physical abuse” OR “sexual abuse” OR “emotional neglect” OR “physical neglect” AND “psychosomatic symptoms” OR “somatization” OR “medically unexplained symptoms” OR somatic symptoms. The inclusion criteria included studies examining traumatic experiences during childhood and adolescence (under 18 years), studies investigating psychosomatic outcomes in adults (18 years and older) childhood trauma measured using standardized assessment tools, including various forms of abuse (physical, sexual, emotional) and neglect (emotional or physical), and psychosomatic symptoms assessed based on the diagnostic and statistical manual of mental disorders, fifth edition (DSM-5) criteria. Additionally, the unavailability of full-text articles and publications in languages other than English was considered an exclusion criterion.
Following the database search, the retrieved articles were imported into EndNote reference management software. Subsequently, titles and abstracts were screened according to the inclusion and exclusion criteria, with irrelevant articles removed. Additionally, the reference lists of identified review articles were examined, and backward citation tracking was performed. Data extraction was conducted independently by two members of the research team. For full-text screening, a standardized checklist was created using Microsoft Excel, including the following fields: first author’s name, publication year, study design, target population, type of childhood trauma assessed, and outcome measures. Studies published in languages other than English, where essential information could not be extracted from abstracts, were excluded from the review process.
Results
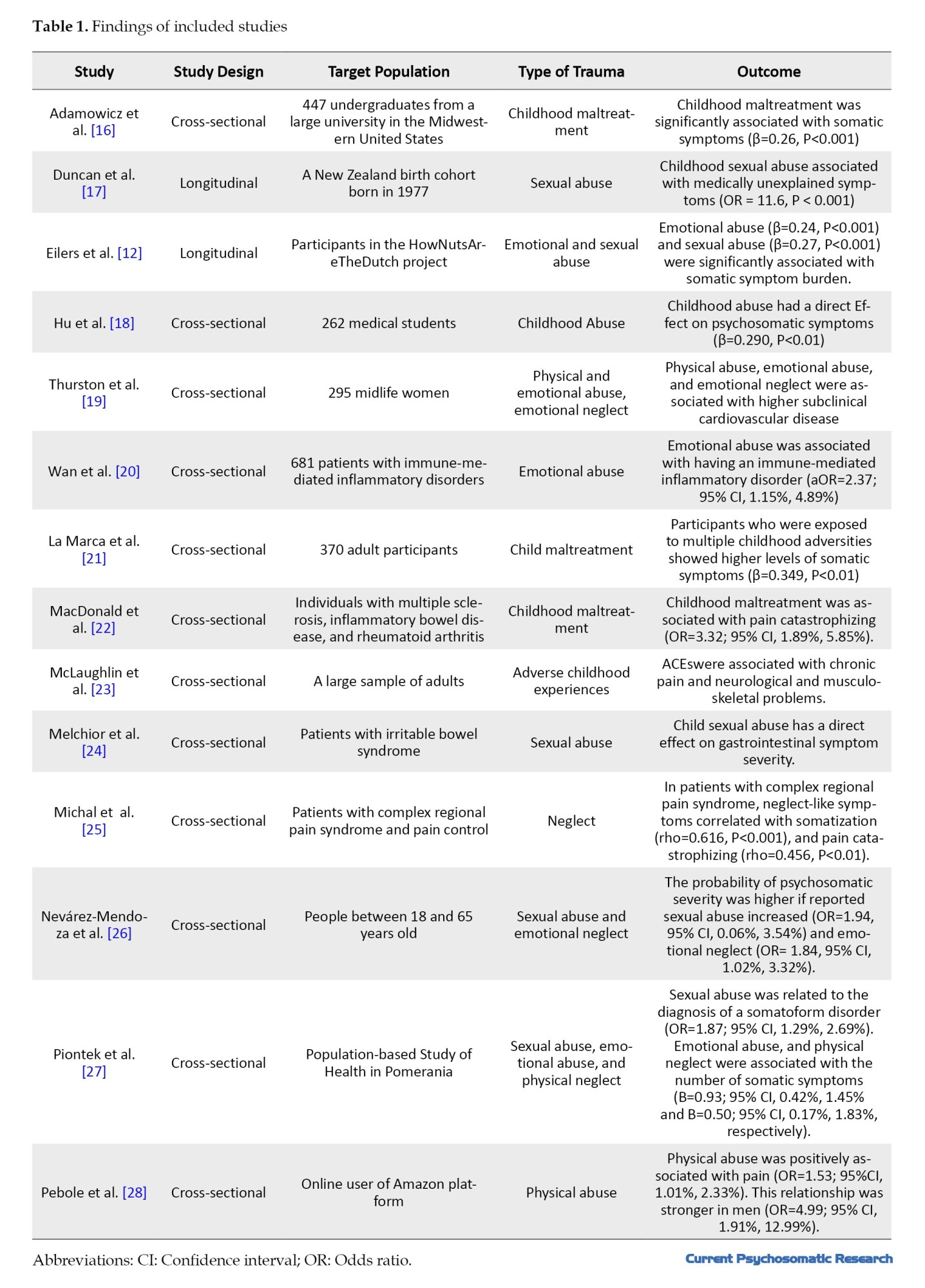
This review included 14 studies published between 2016 and 2024. Two studies employed a longitudinal design (14.3%), while the remaining utilized cross-sectional methodologies (85.7%). The examined samples encompassed diverse populations, including university students, middle-aged women, online users, and individuals with physical health conditions. Regarding the types of trauma assessed: five studies investigated childhood abuse generally (35.7%), five focused on emotional abuse (35.7%), five examined sexual abuse (35.7%), three addressed physical abuse (21.4%), and three studied neglect (21.4%).
This review gathered evidence from multiple studies examining the association between childhood trauma and psychosomatic symptoms across diverse populations. The included studies, comprising both cross-sectional and longitudinal designs, consistently demonstrated that various forms of childhood maltreatment—including emotional, physical, and sexual abuse, as well as neglect—are significantly linked to increased somatic symptom burden. For instance, Adamowicz et al. [16] found childhood maltreatment strongly correlated with psychosomatic symptoms (β=0.26, P<0.001), while Duncan et al. [17] reported a striking association between sexual abuse and medically unexplained symptoms (odds ratio [OR]=11.6, P<0.001). Similarly, Eilers et al. [12] highlighted the impact of emotional and sexual abuse on psychosomatic symptom severity (β=0.24 and 0.27, respectively, P<0.001), reinforcing the pervasive influence of early-life adversity on physical health outcomes.
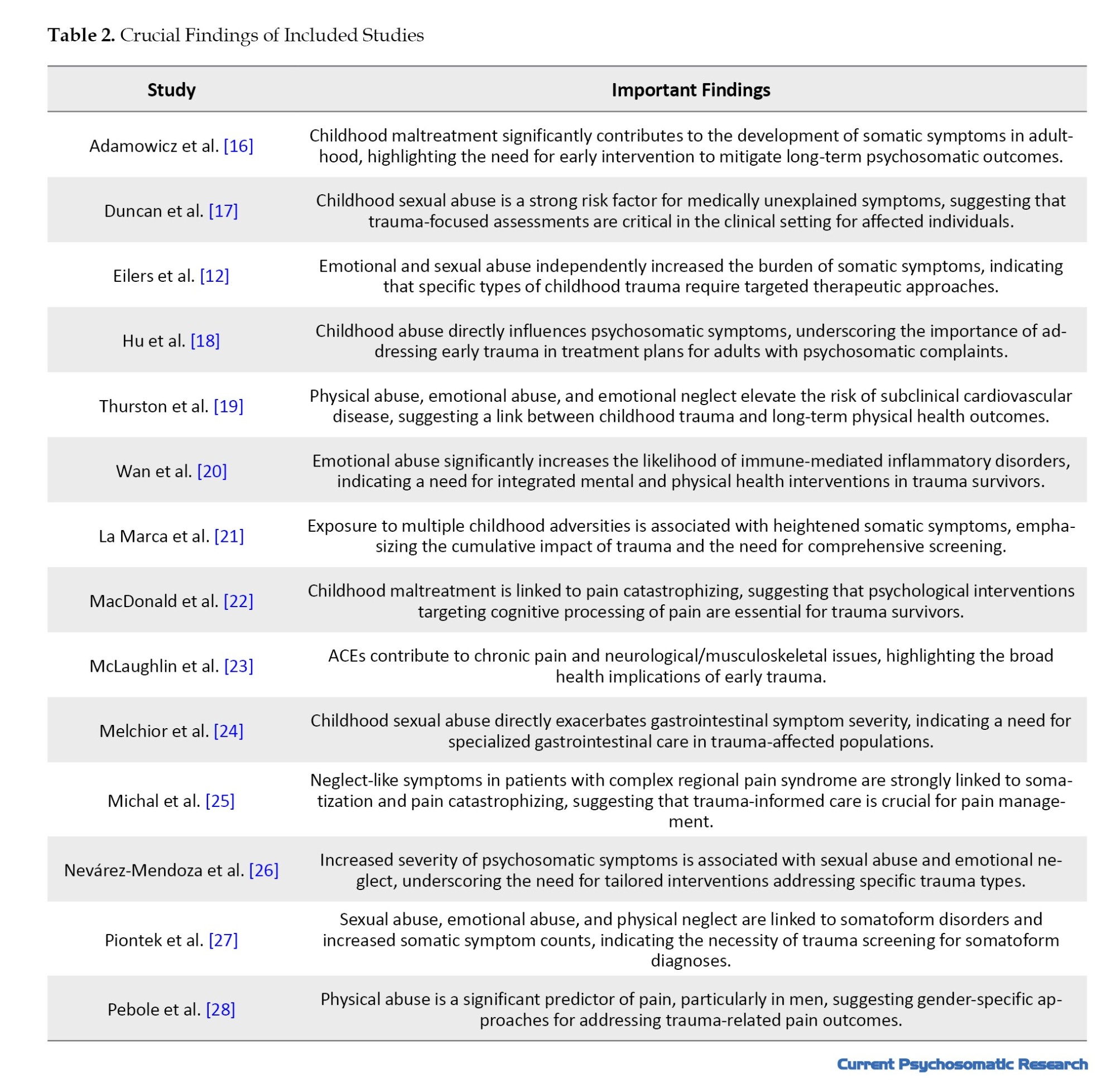
The reviewed studies revealed that childhood trauma is not only associated with general somatic complaints but also with specific medical conditions, including immune-mediated disorders (Wan et al. [20]; aOR=2.37), cardiovascular disease [19], and chronic pain [23]. Notably, MacDonald et al. [22] identified a strong relationship between childhood maltreatment and pain catastrophizing in patients with autoimmune diseases (OR=3.32, 95% confidence interval [CI], 1.89%, 5.85%). Furthermore, emotional neglect and abuse emerged as significant predictors of psychosomatic severity [26], while sexual abuse was specifically tied to somatoform disorders [27]. These findings underscore the need for trauma-informed care in clinical settings, particularly for individuals presenting with medically unexplained symptoms or chronic pain. Tables 1 and 2 presents the crucial findings of the included studies.
Discussion
The findings of this review consistently demonstrate a significant association between childhood trauma, including emotional, physical, and sexual abuse, and neglect, and heightened psychosomatic symptom burden across diverse populations. Beyond general somatic complaints, childhood maltreatment appears to contribute to specific medical conditions, such as immune-mediated disorders, cardiovascular disease, and chronic pain, with emotional neglect and abuse particularly linked to psychosomatic severity. In contrast, sexual abuse shows a distinct connection with somatoform disorders. These results highlight the profound and multifaceted impact of early-life adversity on long-term physical health, emphasizing the importance of trauma-informed approaches in clinical practice, especially for patients presenting with medically unexplained symptoms or persistent pain.
Childhood trauma, including emotional, physical, and sexual abuse as well as neglect, can lead to persistent psychosomatic symptoms through maladaptive psychological mechanisms. Chronic stress in early life disrupts the development of healthy emotional regulation, increasing vulnerability to somatization—a process where psychological distress manifests as physical symptoms. Trauma survivors often develop hypervigilance and heightened bodily awareness, interpreting normal physiological sensations as signs of illness [25]. Additionally, childhood adversity is strongly associated with anxiety and depression, both of which exacerbate somatic complaints, such as chronic pain, fatigue, and gastrointestinal disturbances. The lack of secure attachment in abusive or neglectful environments further impairs coping strategies, leaving individuals more prone to expressing psychological distress through somatic channels.
Exposure to chronic stress during childhood can induce long-term neurobiological changes that predispose individuals to psychosomatic disorders. The HPA axis, which regulates stress responses, becomes dysregulated following prolonged trauma, leading to either hyper- or hypoactivity in cortisol production. This dysregulation contributes to systemic inflammation, a key factor in conditions, such as fibromyalgia, irritable bowel syndrome, and autoimmune disorders [20]. Furthermore, early trauma can alter brain structure and function, particularly in the amygdala (involved in fear processing) and prefrontal cortex (responsible for emotional regulation). These changes may heighten pain perception and lower pain tolerance, explaining the strong association between childhood maltreatment and chronic pain syndrome. Epigenetic modifications due to trauma may also play a role, silencing or activating genes related to stress reactivity and immune function, further embedding somatic vulnerability [22].
Childhood trauma shapes cognitive and behavioral responses in ways that perpetuate psychosomatic symptoms. Maladaptive coping mechanisms, such as avoidance or catastrophizing, are common among trauma survivors and can amplify their physical discomfort. For instance, individuals with a history of abuse may develop pain catastrophizing, a cognitive distortion where pain is perceived as overwhelming and uncontrollable, which exacerbates symptom severity [18]. Additionally, trauma survivors often exhibit somatization as a means of expressing distress when verbalizing emotions feels unsafe or inaccessible. This is particularly evident in cultures where somatic complaints are more socially acceptable than psychological ones. The learned association between stress and physical symptoms can create a feedback loop, wherein health anxiety further intensifies bodily sensations, leading to increased healthcare utilization without clear medical explanations [26].
Also, extensive research has demonstrated that childhood trauma induces persistent dysregulation of the body’s stress response systems, leading to tangible physiological consequences. Chronic activation of the HPA axis and sympathetic nervous system results in prolonged exposure to stress hormones, such as cortisol and adrenaline. Over time, this hormonal imbalance contributes to systemic inflammation, a known precursor to various medical conditions. Specifically, the sustained inflammatory state triggered by early trauma helps explain the increased prevalence of immune-mediated disorders among maltreated individuals, as the immune system remains in a heightened state of alert [20]. This biological embedding of stress may account for the development of autoimmune conditions and allergic disorders, as well as increased susceptibility to infections later in life.
The relationship between childhood trauma and cardiovascular disease emerges through multiple interconnected pathways. Chronic stress during childhood leads to endothelial dysfunction, arterial stiffness, and elevated blood pressure, which are early markers of cardiovascular risk. Furthermore, trauma survivors often develop maladaptive coping behaviors such as smoking, poor diet, and physical inactivity that compound this risk. The persistent inflammatory state mentioned earlier also accelerates atherosclerosis progression. Notably, studies have found that individuals with childhood trauma histories frequently exhibit dysregulated autonomic nervous system function, characterized by reduced heart rate variability, a strong predictor of future cardiovascular events [19]. These findings suggest that the cardiovascular system may be particularly vulnerable to the long-term effects of early life stress.
The association between childhood maltreatment and chronic pain disorders reflects profound alterations in pain processing systems. Early trauma appears to induce central sensitization, a condition where the nervous system becomes hyperreactive to pain signals. Neuroimaging studies have revealed that abused individuals often show structural and functional changes in brain regions involved in pain perception and modulation, including the anterior cingulate cortex and insula [23]. Additionally, the constant stress from maltreatment may lead to muscle tension and myofascial pain through sustained sympathetic activation. The high prevalence of conditions, such as fibromyalgia, chronic back pain, and headaches, among trauma survivors suggests that early adversity may permanently lower pain thresholds and impair endogenous pain inhibition mechanisms [24].
The strong relationship between childhood trauma and psychosomatic symptoms underscores the need for trauma-informed care in medical and psychological practice. Traditional biomedical approaches that focus solely on symptom management often fail to address the root causes of somatic distress in trauma survivors. Instead, integrated treatments—such as cognitive-behavioral therapy, mindfulness-based stress reduction, and somatic experiencing—can help patients process trauma while reducing physical symptoms. Clinicians should routinely screen for adverse childhood experiences (ACEs) in patients with unexplained medical conditions, as early identification of trauma can guide more effective interventions. Furthermore, fostering secure therapeutic relationships can help trauma survivors develop healthier emotional expression and coping strategies, ultimately reducing reliance on somatic symptoms as a means of communicating distress. Future research should explore personalized interventions targeting the specific pathways (psychological, neurobiological, and behavioral) through which trauma influences somatic health.
Conclusion
These findings necessitate a paradigm shift in how we approach chronic medical conditions, urging clinicians to consider the history of childhood trauma as a potential contributing factor. Evidence supports the implementation of routine trauma screening in patients presenting with immune disorders, cardiovascular disease, or chronic pain. Treatment approaches should incorporate trauma-informed care principles while addressing both psychological and physiological dimensions of these conditions. Future research should focus on identifying resilience factors that may mitigate trauma’s physical health consequences and developing targeted interventions that address the specific biological pathways affected by early adversity. This could include mind-body therapies, anti-inflammatory approaches, and interventions that restore autonomic nervous system balance, potentially interrupting the trajectory from childhood trauma to chronic disease.
Although the evidence is robust, the predominance of cross-sectional designs limits causal inference, underscoring the necessity for longitudinal and interventional research. Another limitation of this study is that the quality of the included studies was not assessed. Additionally, since the samples in the included studies consisted of individuals over 18 years old, psychosomatic or physical symptoms may be influenced by aging, which complicates establishing a causal relationship with childhood maltreatment. Furthermore, the use of various statistical indices, such as OR, r, and β coefficients, across the included studies makes comparisons challenging. Different tools were used to measure childhood maltreatment, and the variability in findings limits the ability to integrate results. Additionally, variations in measurement tools and population characteristics (e.g. medical students, midlife women, and patients with chronic illnesses) suggest that findings may not be universally generalizable. Future studies should explore mechanistic pathways—such as dysregulated stress responses or inflammatory processes—to elucidate how childhood trauma translates into somatic morbidity. Addressing these gaps could inform targeted interventions to mitigate the long-term health consequences of early-life adversity.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
Asubstantial body of research in psychosomatic medicine demonstrates that various somatic conditions can emerge as direct consequences of psychological disturbances, highlighting the intricate mind-body interconnection [1]. Prolonged exposure to chronic stress, persistent anxiety, and unprocessed traumatic experiences can induce significant dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, subsequently triggering a cascade of pathophysiological alterations [2]. At the neurobiological level, this psychophysiological interplay is mediated through aberrant neurotransmitter signaling and dysfunction within the autonomic nervous system [3]. Empirical evidence further reveals that depressive disorders are associated with elevated levels of proinflammatory cytokines, which may potentiate cardiovascular pathology, whereas somatization disorders frequently present with medically unexplained physical symptoms in the absence of a detectable organic etiology. These findings collectively underscore the propensity for psychological distress to translate into somatic manifestations [4].
Psychosomatic symptoms represent a complex interplay between psychological distress and physiological manifestations, where emotional or cognitive factors directly contribute to physical dysfunction without clear organic pathology [4]. These symptoms often manifest as gastrointestinal disturbances (e.g. irritable bowel syndrome) or cardiovascular irregularities (e.g. hypertension), mediated by dysregulated stress responses via the HPA axis and autonomic nervous system overactivation [5]. Neuroimaging studies implicate altered activity in limbic regions (e.g. the amygdala and anterior cingulate cortex) that modulate pain perception and visceral sensitivity. Notably, conditions, such as conversion disorder, demonstrate symptom specificity (e.g. paralysis, pseudoseizures), reflecting subconscious psychological conflicts [6].
Psychosomatic symptoms can precipitate a cascade of debilitating physiological and psychological consequences, creating a vicious cycle of impairment [7]. Medically unexplained symptoms (e.g. chronic pain, fatigue, or gastrointestinal distress) often lead to repeated, fruitless medical investigations, fostering patient frustration and eroding trust in healthcare systems [8]. Psychologically, these symptoms correlate with heightened anxiety and depressive disorders due to persistent distress and perceived loss of bodily control. Cognitive distortions, such as catastrophic thinking or health-related hypervigilance, may develop, exacerbating symptom severity and functional disability [9]. Socially, individuals frequently experience stigmatization—dismissed as “fabricating” illness—which compounds isolation and reduces treatment adherence [10]. Over time, the chronicity of psychosomatic conditions can induce maladaptive coping strategies (e.g. avoidance behaviors), further entrenching mind-body dysfunction, and diminishing quality of life [11].
Given the aforementioned consequences, identifying the contributing factors to psychosomatic symptoms would be highly beneficial for preventive interventions. Childhood trauma can precipitate the development of psychosomatic symptoms through persistent maladaptive changes in neurobiological stress-response systems and emotional processing pathways [12]. Early adverse experiences (e.g. abuse, neglect) induce chronic hyperactivity of the HPA axis, leading to prolonged cortisol exposure that disrupts immune function and promotes systemic inflammation [13]. Concurrently, trauma alters limbic system connectivity (particularly amygdala hyperactivity and prefrontal cortex dysregulation), impairing affect modulation and amplifying interoceptive sensitivity to bodily sensations [13]. These neurophysiological adaptations manifest as heightened somatic awareness and dysfunctional autonomic nervous system responses, wherein psychological distress becomes somatized with chronic pain, gastrointestinal disturbances, or conversion symptoms [14]. Furthermore, trauma-related dissociation may fragment the cognitive processing of emotional distress, redirecting it through somatic channels [14]. Epigenetic modifications of stress-related genes and enduring attachment disruptions further entrench this mind-body dysregulation, creating a diathesis for psychosomatic disorders that often persist into adulthood [15].
This narrative review is critically needed to synthesize the growing yet disparate body of evidence linking childhood trauma to adult psychosomatic pathology, while addressing significant gaps in current understanding. This study’s innovation lies in its interdisciplinary approach—bridging developmental psychopathology and psychoneuroimmunology to propose a unified biopsychosocial model of trauma-induced somatization. It addresses explicitly under-researched areas, such as the dose-response relationship between trauma subtypes (emotional vs physical abuse) and specific somatic symptom clusters, as well as protective resilience factors.
Materials and Methods
This study employed a narrative (non-systematic) review methodology, as this approach offers flexibility in synthesizing findings from studies with diverse designs and enables qualitative analysis. The inclusion criteria encompassed primary research investigating the role of childhood trauma in the development of psychosomatic symptoms in adulthood. Accordingly, all eligible cross-sectional, cohort, and other relevant studies were included. A comprehensive search was conducted across four international databases (Web of Science, PubMed, Scopus, and Google Scholar) for publications from 2016 to 2025. Additionally, the reference lists of all selected review articles identified in the initial screening phase were thoroughly examined to ensure comprehensive coverage of relevant literature (Figure1).
The search was conducted using combined keywords of “childhood trauma” OR “childhood trauma” OR “child maltreatment” OR “child abuse” OR “childhood adversity” OR “adverse childhood experiences” OR “emotional abuse” OR “psychological abuse” OR “physical abuse” OR “sexual abuse” OR “emotional neglect” OR “physical neglect” AND “psychosomatic symptoms” OR “somatization” OR “medically unexplained symptoms” OR somatic symptoms. The inclusion criteria included studies examining traumatic experiences during childhood and adolescence (under 18 years), studies investigating psychosomatic outcomes in adults (18 years and older) childhood trauma measured using standardized assessment tools, including various forms of abuse (physical, sexual, emotional) and neglect (emotional or physical), and psychosomatic symptoms assessed based on the diagnostic and statistical manual of mental disorders, fifth edition (DSM-5) criteria. Additionally, the unavailability of full-text articles and publications in languages other than English was considered an exclusion criterion.
Following the database search, the retrieved articles were imported into EndNote reference management software. Subsequently, titles and abstracts were screened according to the inclusion and exclusion criteria, with irrelevant articles removed. Additionally, the reference lists of identified review articles were examined, and backward citation tracking was performed. Data extraction was conducted independently by two members of the research team. For full-text screening, a standardized checklist was created using Microsoft Excel, including the following fields: first author’s name, publication year, study design, target population, type of childhood trauma assessed, and outcome measures. Studies published in languages other than English, where essential information could not be extracted from abstracts, were excluded from the review process.
Results
This review included 14 studies published between 2016 and 2024. Two studies employed a longitudinal design (14.3%), while the remaining utilized cross-sectional methodologies (85.7%). The examined samples encompassed diverse populations, including university students, middle-aged women, online users, and individuals with physical health conditions. Regarding the types of trauma assessed: five studies investigated childhood abuse generally (35.7%), five focused on emotional abuse (35.7%), five examined sexual abuse (35.7%), three addressed physical abuse (21.4%), and three studied neglect (21.4%).
This review gathered evidence from multiple studies examining the association between childhood trauma and psychosomatic symptoms across diverse populations. The included studies, comprising both cross-sectional and longitudinal designs, consistently demonstrated that various forms of childhood maltreatment—including emotional, physical, and sexual abuse, as well as neglect—are significantly linked to increased somatic symptom burden. For instance, Adamowicz et al. [16] found childhood maltreatment strongly correlated with psychosomatic symptoms (β=0.26, P<0.001), while Duncan et al. [17] reported a striking association between sexual abuse and medically unexplained symptoms (odds ratio [OR]=11.6, P<0.001). Similarly, Eilers et al. [12] highlighted the impact of emotional and sexual abuse on psychosomatic symptom severity (β=0.24 and 0.27, respectively, P<0.001), reinforcing the pervasive influence of early-life adversity on physical health outcomes.
The reviewed studies revealed that childhood trauma is not only associated with general somatic complaints but also with specific medical conditions, including immune-mediated disorders (Wan et al. [20]; aOR=2.37), cardiovascular disease [19], and chronic pain [23]. Notably, MacDonald et al. [22] identified a strong relationship between childhood maltreatment and pain catastrophizing in patients with autoimmune diseases (OR=3.32, 95% confidence interval [CI], 1.89%, 5.85%). Furthermore, emotional neglect and abuse emerged as significant predictors of psychosomatic severity [26], while sexual abuse was specifically tied to somatoform disorders [27]. These findings underscore the need for trauma-informed care in clinical settings, particularly for individuals presenting with medically unexplained symptoms or chronic pain. Tables 1 and 2 presents the crucial findings of the included studies.
Discussion
The findings of this review consistently demonstrate a significant association between childhood trauma, including emotional, physical, and sexual abuse, and neglect, and heightened psychosomatic symptom burden across diverse populations. Beyond general somatic complaints, childhood maltreatment appears to contribute to specific medical conditions, such as immune-mediated disorders, cardiovascular disease, and chronic pain, with emotional neglect and abuse particularly linked to psychosomatic severity. In contrast, sexual abuse shows a distinct connection with somatoform disorders. These results highlight the profound and multifaceted impact of early-life adversity on long-term physical health, emphasizing the importance of trauma-informed approaches in clinical practice, especially for patients presenting with medically unexplained symptoms or persistent pain.
Childhood trauma, including emotional, physical, and sexual abuse as well as neglect, can lead to persistent psychosomatic symptoms through maladaptive psychological mechanisms. Chronic stress in early life disrupts the development of healthy emotional regulation, increasing vulnerability to somatization—a process where psychological distress manifests as physical symptoms. Trauma survivors often develop hypervigilance and heightened bodily awareness, interpreting normal physiological sensations as signs of illness [25]. Additionally, childhood adversity is strongly associated with anxiety and depression, both of which exacerbate somatic complaints, such as chronic pain, fatigue, and gastrointestinal disturbances. The lack of secure attachment in abusive or neglectful environments further impairs coping strategies, leaving individuals more prone to expressing psychological distress through somatic channels.
Exposure to chronic stress during childhood can induce long-term neurobiological changes that predispose individuals to psychosomatic disorders. The HPA axis, which regulates stress responses, becomes dysregulated following prolonged trauma, leading to either hyper- or hypoactivity in cortisol production. This dysregulation contributes to systemic inflammation, a key factor in conditions, such as fibromyalgia, irritable bowel syndrome, and autoimmune disorders [20]. Furthermore, early trauma can alter brain structure and function, particularly in the amygdala (involved in fear processing) and prefrontal cortex (responsible for emotional regulation). These changes may heighten pain perception and lower pain tolerance, explaining the strong association between childhood maltreatment and chronic pain syndrome. Epigenetic modifications due to trauma may also play a role, silencing or activating genes related to stress reactivity and immune function, further embedding somatic vulnerability [22].
Childhood trauma shapes cognitive and behavioral responses in ways that perpetuate psychosomatic symptoms. Maladaptive coping mechanisms, such as avoidance or catastrophizing, are common among trauma survivors and can amplify their physical discomfort. For instance, individuals with a history of abuse may develop pain catastrophizing, a cognitive distortion where pain is perceived as overwhelming and uncontrollable, which exacerbates symptom severity [18]. Additionally, trauma survivors often exhibit somatization as a means of expressing distress when verbalizing emotions feels unsafe or inaccessible. This is particularly evident in cultures where somatic complaints are more socially acceptable than psychological ones. The learned association between stress and physical symptoms can create a feedback loop, wherein health anxiety further intensifies bodily sensations, leading to increased healthcare utilization without clear medical explanations [26].
Also, extensive research has demonstrated that childhood trauma induces persistent dysregulation of the body’s stress response systems, leading to tangible physiological consequences. Chronic activation of the HPA axis and sympathetic nervous system results in prolonged exposure to stress hormones, such as cortisol and adrenaline. Over time, this hormonal imbalance contributes to systemic inflammation, a known precursor to various medical conditions. Specifically, the sustained inflammatory state triggered by early trauma helps explain the increased prevalence of immune-mediated disorders among maltreated individuals, as the immune system remains in a heightened state of alert [20]. This biological embedding of stress may account for the development of autoimmune conditions and allergic disorders, as well as increased susceptibility to infections later in life.
The relationship between childhood trauma and cardiovascular disease emerges through multiple interconnected pathways. Chronic stress during childhood leads to endothelial dysfunction, arterial stiffness, and elevated blood pressure, which are early markers of cardiovascular risk. Furthermore, trauma survivors often develop maladaptive coping behaviors such as smoking, poor diet, and physical inactivity that compound this risk. The persistent inflammatory state mentioned earlier also accelerates atherosclerosis progression. Notably, studies have found that individuals with childhood trauma histories frequently exhibit dysregulated autonomic nervous system function, characterized by reduced heart rate variability, a strong predictor of future cardiovascular events [19]. These findings suggest that the cardiovascular system may be particularly vulnerable to the long-term effects of early life stress.
The association between childhood maltreatment and chronic pain disorders reflects profound alterations in pain processing systems. Early trauma appears to induce central sensitization, a condition where the nervous system becomes hyperreactive to pain signals. Neuroimaging studies have revealed that abused individuals often show structural and functional changes in brain regions involved in pain perception and modulation, including the anterior cingulate cortex and insula [23]. Additionally, the constant stress from maltreatment may lead to muscle tension and myofascial pain through sustained sympathetic activation. The high prevalence of conditions, such as fibromyalgia, chronic back pain, and headaches, among trauma survivors suggests that early adversity may permanently lower pain thresholds and impair endogenous pain inhibition mechanisms [24].
The strong relationship between childhood trauma and psychosomatic symptoms underscores the need for trauma-informed care in medical and psychological practice. Traditional biomedical approaches that focus solely on symptom management often fail to address the root causes of somatic distress in trauma survivors. Instead, integrated treatments—such as cognitive-behavioral therapy, mindfulness-based stress reduction, and somatic experiencing—can help patients process trauma while reducing physical symptoms. Clinicians should routinely screen for adverse childhood experiences (ACEs) in patients with unexplained medical conditions, as early identification of trauma can guide more effective interventions. Furthermore, fostering secure therapeutic relationships can help trauma survivors develop healthier emotional expression and coping strategies, ultimately reducing reliance on somatic symptoms as a means of communicating distress. Future research should explore personalized interventions targeting the specific pathways (psychological, neurobiological, and behavioral) through which trauma influences somatic health.
Conclusion
These findings necessitate a paradigm shift in how we approach chronic medical conditions, urging clinicians to consider the history of childhood trauma as a potential contributing factor. Evidence supports the implementation of routine trauma screening in patients presenting with immune disorders, cardiovascular disease, or chronic pain. Treatment approaches should incorporate trauma-informed care principles while addressing both psychological and physiological dimensions of these conditions. Future research should focus on identifying resilience factors that may mitigate trauma’s physical health consequences and developing targeted interventions that address the specific biological pathways affected by early adversity. This could include mind-body therapies, anti-inflammatory approaches, and interventions that restore autonomic nervous system balance, potentially interrupting the trajectory from childhood trauma to chronic disease.
Although the evidence is robust, the predominance of cross-sectional designs limits causal inference, underscoring the necessity for longitudinal and interventional research. Another limitation of this study is that the quality of the included studies was not assessed. Additionally, since the samples in the included studies consisted of individuals over 18 years old, psychosomatic or physical symptoms may be influenced by aging, which complicates establishing a causal relationship with childhood maltreatment. Furthermore, the use of various statistical indices, such as OR, r, and β coefficients, across the included studies makes comparisons challenging. Different tools were used to measure childhood maltreatment, and the variability in findings limits the ability to integrate results. Additionally, variations in measurement tools and population characteristics (e.g. medical students, midlife women, and patients with chronic illnesses) suggest that findings may not be universally generalizable. Future studies should explore mechanistic pathways—such as dysregulated stress responses or inflammatory processes—to elucidate how childhood trauma translates into somatic morbidity. Addressing these gaps could inform targeted interventions to mitigate the long-term health consequences of early-life adversity.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
- Grigorian K, Östberg V, Raninen J, Åhlén J, Brolin Låftman S. Prospective associations between psychosomatic complaints in adolescence and depression and anxiety symptoms in young adulthood: A Swedish national cohort study. SSM Popul Health. 2023; 24:101509. [DOI:10.1016/j.ssmph.2023.101509] [PMID]
- Wöhrmann AM, Ebner C. Understanding the bright side and the dark side of telework: An empirical analysis of working conditions and psychosomatic health complaints. N Technol Work Employ. 2021; 36(3):348-70. [DOI:10.1111/ntwe.12208]
- Zidkova R, Malinakova K, van Dijk JP, Tavel P. The coronavirus pandemic and the occurrence of psychosomatic symptoms: Are they related? Int J Environ Res Public Health. 2021; 18(7):3570. [DOI:10.3390/ijerph18073570] [PMID]
- Brooks SJ, Titova OE, Ashworth EL, Bylund SBA, Feldman I, Schiöth HB. Self-reported psychosomatic complaints and conduct problems in Swedish adolescents. Children. 2022; 9(7):963. [DOI:10.3390/children9070963] [PMID]
- Shukla M, Upadhyay N. Psychosomatic problems among adolescents during/post the COVID-19 pandemic: A systematic review. Adolesc Psychiatry. 2024; 14(3):134-63. [DOI:10.2174/0122106766307916240626104350]
- Kano M, Van Oudenhove L, Dupont P, Wager TD, Fukudo S. Imaging brain mechanisms of functional somatic syndromes: potential as a biomarker? Tohoku J Exp Med. 2020; 250(3):137-52. [DOI:10.1620/tjem.250.137] [PMID]
- Tatayeva R, Ossadchaya E, Sarculova S, Sembayeva Z, Koigeldinova S. Psychosomatic aspects of the development of comorbid pathology: A review. Med J Islam Repub Iran. 2022; 36:152. [DOI:10.47176/mjiri.36.152] [PMID]
- Fava GA, Cosci F, Sonino N. Current psychosomatic practice. Psychother Psychosom. 2017; 86(1):13-30. [DOI:10.1159/000448856] [PMID]
- Gasparre D, Pepe I, Laera D, Abbatantuono C, De Caro MF, Taurino A, et al. Cognitive functioning and psychosomatic syndromes in a subjective tinnitus sample. Front Psychol. 2023; 14:1256291. [DOI:10.3389/fpsyg.2023.1256291] [PMID]
- Tawfellos G, Torosoff M. The psychosomatic impacts of social isolation on cardiac disease symptom frequency and severity. Int J Cardiol. 2022; 366:50. [DOI:10.1016/j.ijcard.2022.07.003] [PMID]
- Bulut S, Bukhori B, Bhat R. The Experience of Psychosomatic Disorders among Adolescents: Challenges and coping strategies. J Pers Psychosom Res. 2024; 2(2):19-25. [DOI:10.61838/kman.jppr.2.2.4]
- Eilers H, Aan Het Rot M, Jeronimus BF. Childhood trauma and adult somatic symptoms. Psychosom Med. 2023; 85(5):408-416. [DOI:10.1097/PSY.0000000000001208] [PMID]
- Fischer S, Ali N, Feneberg AC, Mewes R, Nater UM. Does childhood trauma impact daily psychobiological stress in somatic symptom disorder? An ambulatory assessment study. Front Psychiatry. 2022; 13:954051. [DOI:10.3389/fpsyt.2022.954051] [PMID]
- Lüönd AM, Ayas G, Bachem R, Carranza-Neira J, Eberle DJ, Fares-Otero NE, et al. Childhood maltreatment and somatic symptoms in adulthood: Establishing a new research pathway. Neuropsychobiology. 2025; 84(2):113-20. [DOI:10.1159/000543438] [PMID]
- Afshari A, Jondi Z. [The role of child’s self-efficacy in the relationship between childhood traumatic events and psychosomatic complaints (Persian)]. J Psychol Stud. 2021; 17(2):139-62. [DOI:10.22051/psy.2021.34386.2375]
- Adamowicz JL, Sirotiak Z, Thomas EBK. Childhood maltreatment and somatic symptoms: Examining the role of specific types of childhood maltreatment and alexithymia. Psychol Trauma. 2024; 16(Suppl 1):S2-9. [DOI:10.1037/tra0001315] [PMID]
- Duncan R, Mulder R, Wilkinson SH, Horwood J. Medically unexplained symptoms and antecedent sexual abuse: An observational study of a birth cohort. Psychosom Med. 2019; 81(7):622-8. [DOI:10.1097/PSY.0000000000000726] [PMID]
- Hu Y, Zhu X, Geng D, Qiao J, Zhou Q, Liu Y, et al. Effect of childhood abuse on psychosomatic symptoms among medical students: Mediating effect of trait coping styles. Chinese J Behav Med Brain Sci. 2018; 2018(12):439-43. [DOI:10.3760/cma.j.issn.1674-6554.2018.05.012]
- Thurston RC, Chang Y, Barinas-Mitchell E, von Känel R, Jennings JR, Santoro N, et al. Child abuse and neglect and subclinical cardiovascular disease among midlife women. Psychosom Med. 2017; 79(4):441-9. [DOI:10.1097/PSY.0000000000000400] [PMID]
- Wan A, Bernstein CN, Graff LA, Patten SB, Sareen J, Fisk JD, et al. Childhood maltreatment and psychiatric comorbidity in immune-mediated inflammatory disorders. Psychosom Med. 2022; 84(1):10-19. [DOI:10.1097/PSY.0000000000001025] [PMID]
- La Marca L, Scalabrini A, Mucci C, Schimmenti A. Traumatic memories and the body: A study on child maltreatment, interoceptive awareness, and somatic symptoms. Maltrattamento E Abuso All’infanzia. 2018; 2(3):47-71. [DOI:10.3280/MAL2018-003004]
- MacDonald TM, Fisk JD, Bernstein CN, El-Gabalawy R, Hitchon CA, Kornelsen J, et al. The association between childhood maltreatment and pain catastrophizing in individuals with immune-mediated inflammatory diseases. J Psychosom Res. 2021; 145:110479. [DOI:10.1016/j.jpsychores.2021.110479] [PMID]
- McLaughlin KA, Lane RD, Bush NR. Introduction to the special issue of psychosomatic medicine: Mechanisms linking early-life adversity to physical health. Psychosom Med. 2016; 78(9):976-8. [DOI:10.1097/PSY.0000000000000420] [PMID]
- Melchior C, Wilpart K, Midenfjord I, Trindade IA, Törnblom H, Tack JF, Simrén M, Van Oudenhove L. Relationship Between Abuse History and Gastrointestinal and extraintestinal symptom severity in irritable bowel syndrome. Psychosom Med. 2022; 84(9):1021-33. [DOI:10.1097/PSY.0000000000001141] [PMID]
- Michal M, Adler J, Reiner I, Wermke A, Ackermann T, Schlereth T, et al. Association of neglect-like symptoms with anxiety, somatization, and depersonalization in complex regional pain syndrome. Pain Med. 2017; 18(4):764-72. [DOI:10.1093/pm/pnw214] [PMID]
- Nevárez-Mendoza BP, Ochoa-Meza G. Relationship between adverse childhood experiences and the physical and mental health in Mexican adults. Salud Ment. 2022; 45(2):61-9. [DOI:10.17711/SM.0185-3325.2022.009]
- Piontek K, Wiesmann U, Apfelbacher C, Völzke H, Grabe HJ. The association of childhood maltreatment, somatization and health-related quality of life in adult age: Results from a population-based cohort study. Child Abuse Negl. 2021; 120:105226. [DOI:10.1016/j.chiabu.2021.105226] [PMID]
- Pebole MM, Greco CE, Gobin RL, Phillips BN, Strauser DR. Impact of childhood maltreatment on psychosomatic outcomes among men and women with disabilities. Disabil Rehabil. 2022; 44(24):7491-9. [DOI:10.1080/09638288.2021.1998666] [PMID]
Type of Study: Research |
Subject:
Psychology
Received: 2024/07/20 | Accepted: 2024/09/13 | Published: 2024/10/1
Received: 2024/07/20 | Accepted: 2024/09/13 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
