Wed, May 27, 2026
[Archive]
Volume 3, Issue 1 (Autumn 2024)
CPR 2024, 3(1): 41-52 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alidoosti F, Yazdani M. Causal Model of Childhood Trauma and Symptoms of Psychosomatic Disorders With the Mediating Role of Self-critical Rumination. CPR 2024; 3 (1) :41-52
URL: http://cpr.mazums.ac.ir/article-1-149-en.html
URL: http://cpr.mazums.ac.ir/article-1-149-en.html



Department of Psychology, Faculty of Humanities, Khayyam University, Mashhad, Iran.
Full-Text [PDF 747 kb]
(34 Downloads)
| Abstract (HTML) (113 Views)
Full-Text: (20 Views)
Introduction
In recent decades, a new category of illnesses known as psychosomatic disorders has emerged, in which emotional and psychological factors play a significant role in their development. According to the diagnostic and statistical manual of mental disorders [1], psychosomatic disorders encompass a broad range of conditions where physical symptoms constitute the core component [2]. As one of the common psychiatric disorders, psychosomatic illness represents a critical issue concerning both physical and mental health. These conditions often respond poorly to both pharmacological treatments and psychotherapy, resulting in substantial direct and indirect costs [3].
The term psychosomatic disorder is used when an individual presents with physical symptoms that appear to be primarily caused or exacerbated by psychological factors, without sufficient medical explanations. These symptoms often coexist with common medical and psychological issues, where psychological and somatic elements are intricately intertwined [4].
Psychiatric comorbidities are highly prevalent in such patients, with reported prevalence rates ranging from 20% to 67%, depending on the specific illness. Global studies indicate that the prevalence of psychosomatic disorders varies and is influenced by gender, cultural background, ethnicity, and various socio-economic factors [5]. Research conducted in European countries has shown that the prevalence of psychosomatic disorders is 18% in Denmark [6]. 70% among youth, 78% among middle-aged individuals, and 81% among the elderly in the Netherlands, and 22% in the United Kingdom [7].
Psychosomatic symptoms may reflect unresolved psychological pain or traumatic life experiences, significant losses, deep personal injuries, or experiences of dehumanization [8]. Some victims of physical violence report severe physical complaints and illnesses. Overall, many object relations theorists consider early developmental trauma as the root of psychosomatic disorders [9]. Children who experience parental abuse are at greater risk of developing various psychiatric problems, including depression, anxiety, psychosis, and personality disorders [10]. Indeed, trauma is one of the key factors that can trigger psychosomatic symptoms in individuals. Childhood maltreatment significantly undermines a child’s well-being and its effects often extend into adulthood [11].
adverse childhood experiences (ACEs) or childhood trauma refer to critical or deep-rooted events that threaten a child’s physical or emotional well-being. The term was first introduced in the study by Ferrari et al. [12] and encompasses a wide range of abusive experiences, including physical abuse, sexual abuse, emotional abuse, as well as neglect, such as physical and emotional neglect. It also includes experiences such as family dysfunction, lack of emotional and educational support, being raised by a family member with a mental illness, parental divorce, or domestic violence [13].
Childhood trauma involves any action or omission by parents or caregivers that causes harm—either overt or covert—or places the child at risk of harm, even if the intent was not to inflict harm [14]. Such experiences may leave the individual feeling vulnerable emotionally, cognitively, and physically, and can adversely affect multiple domains of development, including neurobiological, cognitive, emotional, and general health [15, 16].
Maltreatment causes stress that interferes with early brain development and can disrupt the growth of both the nervous and immune systems. As a result, children who experience maltreatment are at increased risk for behavioral problems, physical health issues, and mental health challenges. In the absence of emotional awareness, these children may indirectly exhibit symptoms of internalizing disorders. Such disorders may manifest as failure to gain expected weight, insomnia or hypersomnia, feelings of worthlessness or excessive guilt, reduced ability to think or concentrate, and recurrent thoughts of death—all of which may overlap with psychosomatic symptoms [17].
Numerous studies have demonstrated a link between childhood trauma and various psychological and physical disorders in adulthood. For instance, Kamandloo et al. [18] found that beyond the widespread cultural emphasis on attractiveness, past trauma and intrapsychic concerns may increase individuals’ sensitivity to rejection and preoccupation with physical appearance. Doba et al. [19] reported that experiencing negative emotions and emotional neglect by caregivers during childhood is associated with alexithymia and increased social isolation in adulthood. Furthermore, physical and emotional abuse in childhood predicts a greater tendency toward self-harming behaviors, aggression, and a reduced capacity for empathy, particularly in intimate relationships in later life [20].
According to the psychosomatic inhibition perspective, the inhibition of thoughts, feelings, or behaviors is accompanied by physiological activity. In the short term, inhibition leads to increased activity of the autonomic nervous system. Over time, inhibition acts as a cumulative stressor that increases the likelihood of developing psychosomatic illnesses.
Actively avoiding thinking or feeling about a trauma, or not talking about it, is considered a particularly harmful form of inhibition. Findings from recent surveys and experiments indicate that childhood traumatic experiences—especially those never discussed—are strongly associated with current physical health problems; recent traumas that have not been discussed are linked to increased physical problems and rumination about the traumas; confronting earlier traumas through writing improves health and immune system functioning; actively talking about distressing experiences is associated with immediate reductions in certain autonomic nervous system activities [21].
One common coping mechanism individuals may adopt in response to traumatic experiences is rumination [22]. There is a significant relationship between childhood trauma and increased levels of rumination in adulthood [23]. Rumination refers to a persistent tendency to think repeatedly about the causes and consequences of negative emotional experiences [24]. Individuals who engage in rumination are more likely to dwell on negative memories, interpret events pessimistically, and, consequently, experience lower life satisfaction and a more negative outlook on life [25].
Rumination exists in various forms, one of which is self-critical rumination. This involves persistent negative self-evaluation, characterized by self-deprecating, judgmental, or pessimistic thoughts related to failures, disappointments, or unattained goals [26]. In this form of rumination, the individual often focuses on perceived worthlessness, shameful aspects of the self, or guilt-inducing thoughts [27, 28]. In general, self-critical individuals tend to believe they have failed in life [29].
Self-critical rumination was a key finding in the study by Sen and Gumus [30], which explained how childhood maltreatment may impair psychological well-being in adulthood. Some studies have also shown that when self-criticism and rumination are combined, self-criticism becomes an even more serious threat to mental well-being [27]. Notably, self-critical rumination significantly predicts self-esteem, even when controlling for age, baseline self-criticism, anxiety, stress, and depression [31]. Persistent and excessive self-criticism, particularly in the form of self-critical rumination, may severely affect an individual’s self-concept, subjective well-being, and overall mental health outcomes [32].
Numerous studies have examined the mediating role of rumination in the relationship between childhood trauma and mental disorders, including study [33], which introduced the response style theory of depression. According to this theory, rumination is an important vulnerability factor for depression that can intensify and prolong depressive episodes [34]. Study also found that a ruminative response style can predict the severity of depression in both clinical and non-clinical samples after one year.
Rumination may contribute to depression by processing and reproducing traumatic childhood experiences. In general, recurring negative thoughts play a significant role in mood disorders and anxiety following a traumatic experience [35]. Another study showed that neuroticism is associated with self-criticism and a general tendency to evaluate oneself negatively. Neuroticism, also known as negative emotionality, is characterized by high sensitivity to negative emotions such as anxiety, anger, and depression, making individuals prone to interpreting events negatively [36].
Longitudinal studies have shown that self-critical rumination predicts future psychopathology (i.e. depressive symptoms, anxiety, or suicidal ideation) [37, 38]. When individuals engage in self-critical rumination, they become trapped in repetitive and persistent thinking about their distress, which can intensify emotional responses (i.e. psychopathology) [28].
Another finding indicated that forgiveness significantly mediates the relationship between childhood trauma and both rumination and intolerance of uncertainty, which in turn significantly mediates the relationship between childhood trauma and social anxiety. Moreover, indirect effects were observed through a sequential pathway from childhood trauma to forgiveness, then to rumination and intolerance of uncertainty, and finally to social anxiety [39].
In another study, it was reported that social stigma directly affects suicidal thoughts and indirectly influences them through deliberate rumination, which mediates 92% of the total effect. These findings suggest that deliberate rumination functions as a cognitive reappraisal mechanism that disrupts the social stigma–suicidality pathway, aligning with the cognitive-behavioral theory’s focus on restructuring maladaptive schemas [40].
But, childhood trauma and maltreatment are among the factors that may contribute to psychosomatic symptoms. Furthermore, childhood trauma may influence the development of such symptoms through mediating variables, such as self-critical rumination. Given the complexity and lack of clarity surrounding the mechanisms and manifestations of psychosomatic disorders, conducting research that seeks to identify and clarify their connections to ACEs and self-critical rumination is of significant importance. Therefore, the present study aims to investigate the following research question: Does self-critical rumination mediate the relationship between childhood trauma and psychosomatic symptoms?
Materials and Methods
This study employed a fundamental research design in terms of purpose and was correlational in terms of data collection, specifically using Path analysis. The statistical population consisted of all adults over 18 years of age in Razavi Khorasan Province between March 2024 and June 2024. According to Schumacher and Lomax’s recommendations for Modeling studies, a sample size between 200 and 600 participants is considered sufficient. Accordingly [41], 300 participants were selected for the current study.
The questionnaires were administered online via the “Porsline” platform and distributed through social media. The inclusion criterion for participants was an age range between 18 and 50 years. Ethical considerations were strictly observed. Along with the questionnaire link, participants received a brief explanation outlining the study’s purpose, assurance of anonymity and confidentiality, and the voluntary nature of participation. Participants were asked to complete the questionnaire only after providing informed consent.
Demographic questionnaire
This section includes questions about gender, age, marital status, employment status, and education.
Childhood trauma questionnaire (CTQ)
Developed by Bernstein et al. [42], the CTQ is suitable for both adults and adolescents. It assesses five types of childhood maltreatment: sexual abuse, physical abuse, emotional abuse, physical neglect, and emotional neglect. The CTQ contains 28 items, of which 25 measure core components and 3 are validity items for identifying individuals who may minimize or deny their traumatic experiences. Higher scores indicate greater levels of trauma. Each subscale ranges from 5 to 25, and the total score ranges from 25 to 125. Previous research reported Cronbach’s α ranging from 0.86 to 0.95 for subscales and construct validity between 0.59 and 0.78. Specifically, the emotional abuse and emotional neglect subscales demonstrated alphas of 0.86 and 0.89, respectively [43]. In this study, the validity of the childhood trauma scale using Cronbach’s α coefficient method was 0.86 for the entire scale and 0.88 for the sexual abuse components, 0.79 for the physical abuse components, 0.81 for the emotional abuse components, 0.86 for the emotional neglect components, and 0.72 for the physical neglect components.
Psychosomatic symptoms questionnaire
Validated by Takata and Sakata [44], this questionnaire consists of 30 items, each rated on a 4-point Likert scale: Never (0), rarely (1), sometimes (2), and frequently (3). The total score ranges from 0 to 90. The authors reported Cronbach’s α between 0.90 and 0.93 across three administrations. Concurrent validity was confirmed through correlation with the Goldberg general health questionnaire, yielding coefficients of 0.64 and 0.65. Construct validity was assessed using factor analysis, with Cronbach’s α values of 0.93 and 0.92. Test-re-test correlations exceeded r=0.5 across three measurements [44]. In this study, the validity of the psychosomatic disorders scale was 0.93.
Self-critical rumination scale (SCRS)
Developed by Smart et al. [27], the SCRS includes 10 items. Items with skewness exceeding three times the standard error were retained due to content importance. Items were derived from both clinical and student samples, as well as existing rumination criteria. The scale uses a 4-point Likert format ranging from 1 (Not at all) to 4 (Very much), with higher scores reflecting greater levels of self-critical rumination. Fearn et al. [28] reported a Cronbach’s α of 0.91, indicating excellent internal consistency. In this study, the validity of the SCRS was 0.90. The collected data were analyzed using SPSS software, version 26 and AMOS software, version 24 at two levels:
Descriptive statistics: Frequency, percentage, Mean±SD. Inferential statistics: Pearson correlation and Path analysis. To examine the normality of the data, according to Chu and Bentler [45], skewness values within ±3 and, based on Kline [46], kurtosis values within ±10 are considered acceptable. In the present study, skewness values (0.20–2.88) and kurtosis values (0.03–9.39) for childhood trauma scores, self-critical rumination, and psychosomatic symptoms were within the acceptable range; therefore, it can be concluded that the data for these variables were normally distributed. In addition, to assess multicollinearity, the variance inflation factor (VIF) and tolerance indices were used. The results indicated that VIF values (1.13–2.75) were below 10, and tolerance values (0.36–0.88) were within the 0–1 range. Thus, it can be stated that no multicollinearity existed among the predictor variables. Furthermore, to ensure that the assumptions of the model were met, the independence of errors was examined using the Durbin–Watson statistic. The obtained value (1.95) for predicting psychosomatic symptoms was less than 4; therefore, it can be concluded that autocorrelation was absent and the assumption of error independence was satisfied.
Results
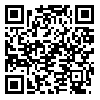
In this study, the majority of participants were female (84.3%), aged 18–25 years (49.7%), held a bachelor’s degree (42.7%), were married (41.7%), and were unemployed (45.7%). Descriptive statistics, including Mean±SD for childhood trauma, self-critical rumination, and psychosomatic symptoms, are presented in Table 1. The mean scores for total childhood trauma, self-critical rumination, and psychosomatic symptoms were 39.93±13.83, 24.22±7.49, and 34.27±16.62, respectively.
Initially, in order to examine the relationship between demographic variables and trauma, the results of the t-test to compare women and men in the trauma score (t=0.52, P=0.598), as well as, the results of the ANOVA test to compare different age groups (F=1.93, P=0.124) and different educational levels (F=0.59, P=0.669) in the scores of this variable were examined, and all of these results indicated no significant difference.
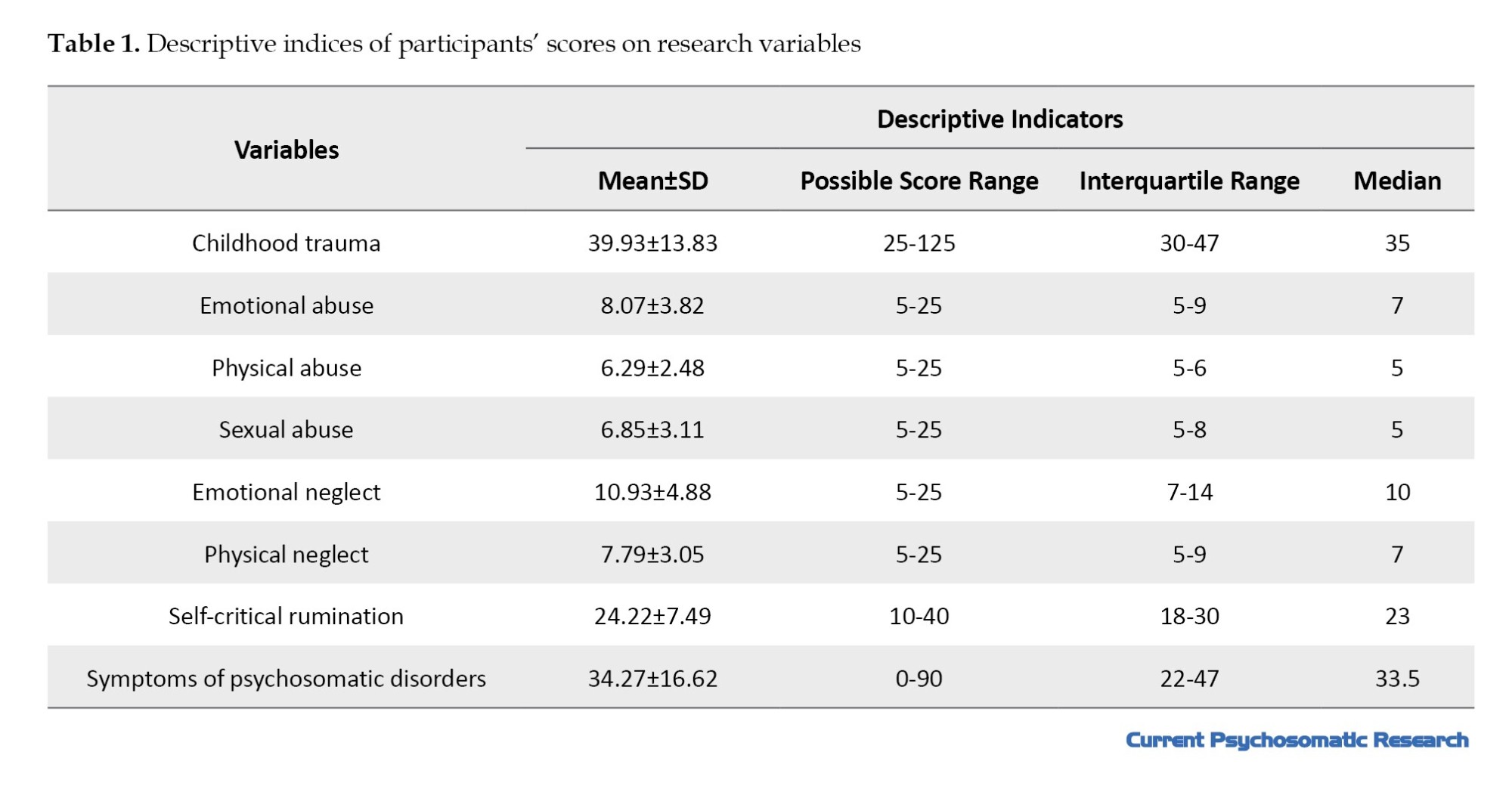
According to the Pearson correlation coefficients presented in Table 2, childhood trauma and all of its components showed a significant positive correlation with psychosomatic symptoms and self-critical rumination.
The positive direction of these correlations indicates that higher levels of childhood trauma and its subcomponents were associated with higher levels of psychosomatic symptoms and self-critical rumination among the study participants.
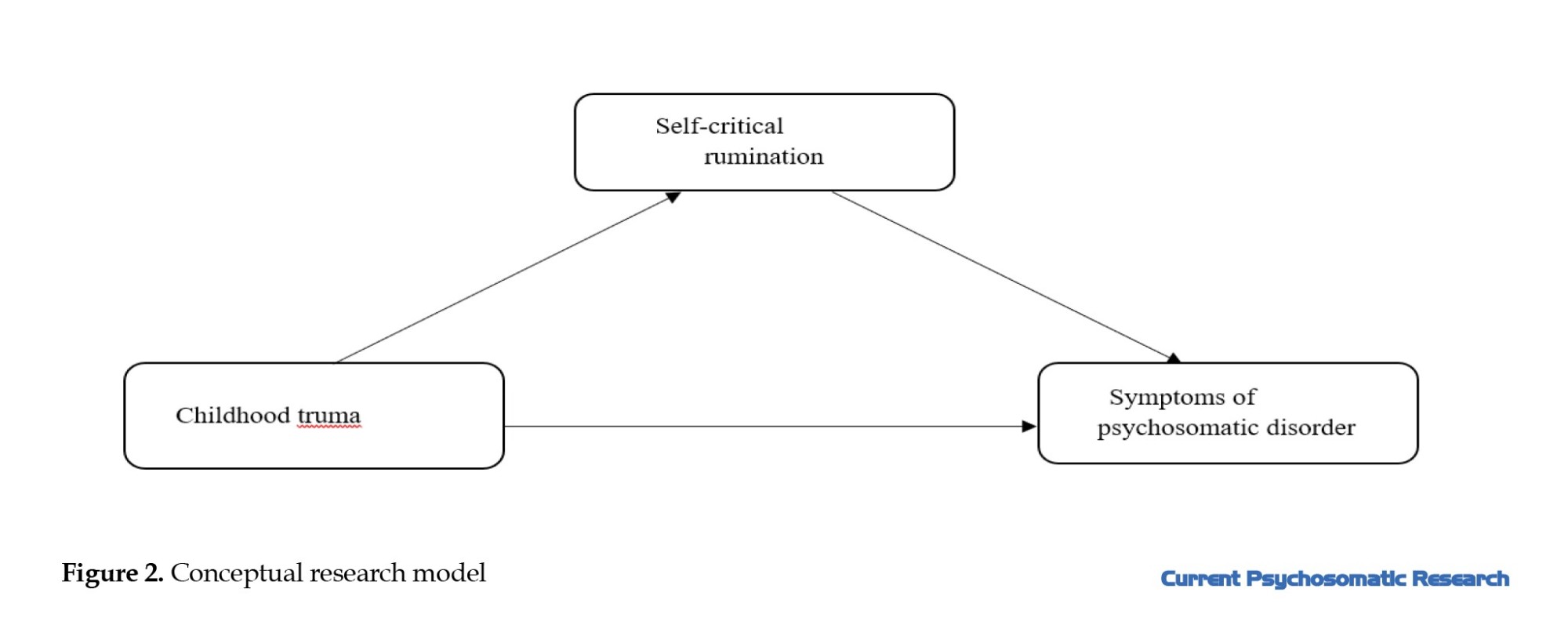
According to this model, childhood trauma was considered as the exogenous latent variable (with observed subcomponents), self-critical rumination served as the mediator, and psychosomatic symptoms were treated as the endogenous variable, with both the mediator and outcome variables being observed variables.
Model fit was evaluated through path analysis using indices such as chi-square (χ²), comparative fit index (CFI), goodness of fit index (GFI), adjusted goodness of fit index (AGFI), and the root mean square error of approximation (RMSEA). For acceptable model fit, the standard criteria are as follows: A chi-square to degrees of freedom ratio (χ²/df) less than 3; CFI, GFI, and AGFI values close to 1; and RMSEA between 0 and 0.05 (indicating a good fit), or between 0.05 and 0.10 (indicating an acceptable fit). Although the chi-square index is commonly used to assess model fit, it tends to increase with larger sample sizes and degrees of freedom; therefore, the RMSEA is recommended as a more robust measure.
Based on these criteria, the overall model fit indices for the initial model were examined. The results indicated a “good” model fit, and the detailed findings are presented below.
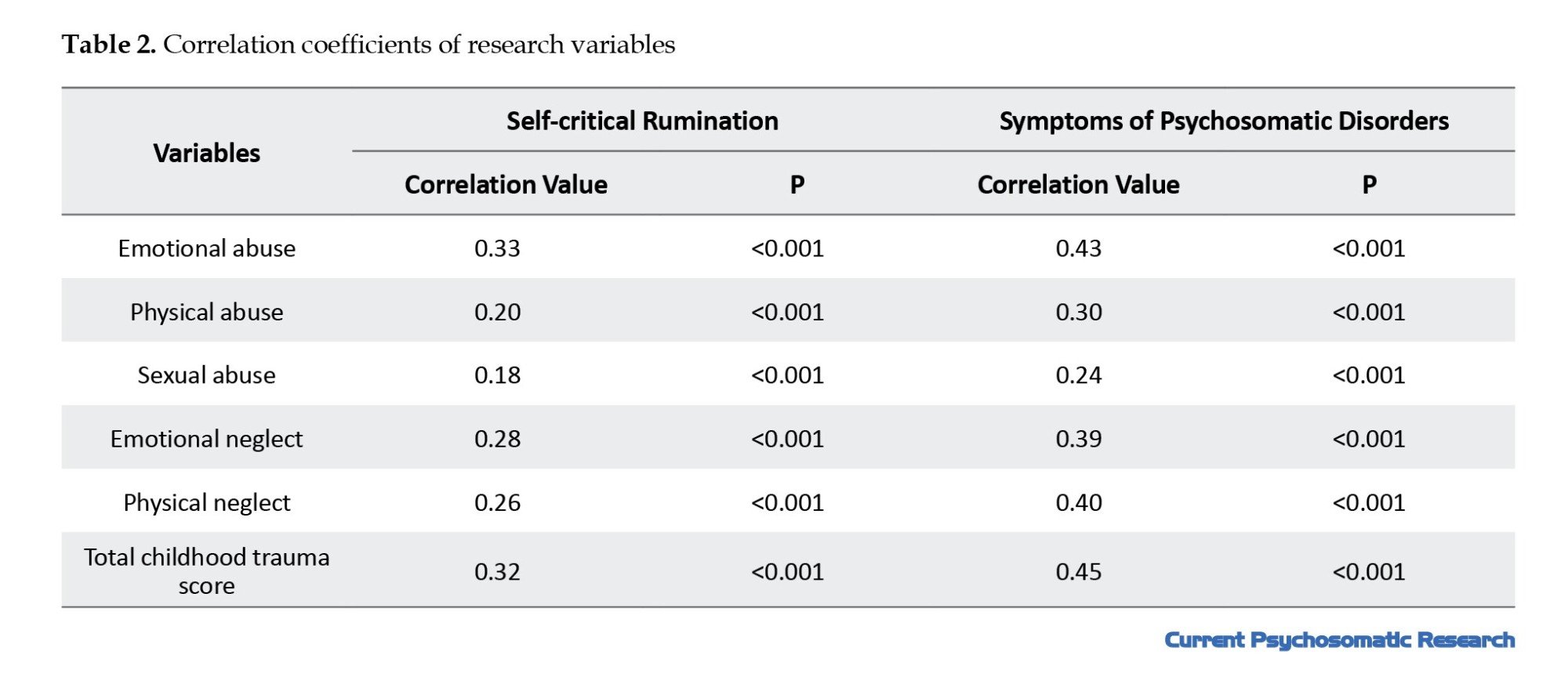
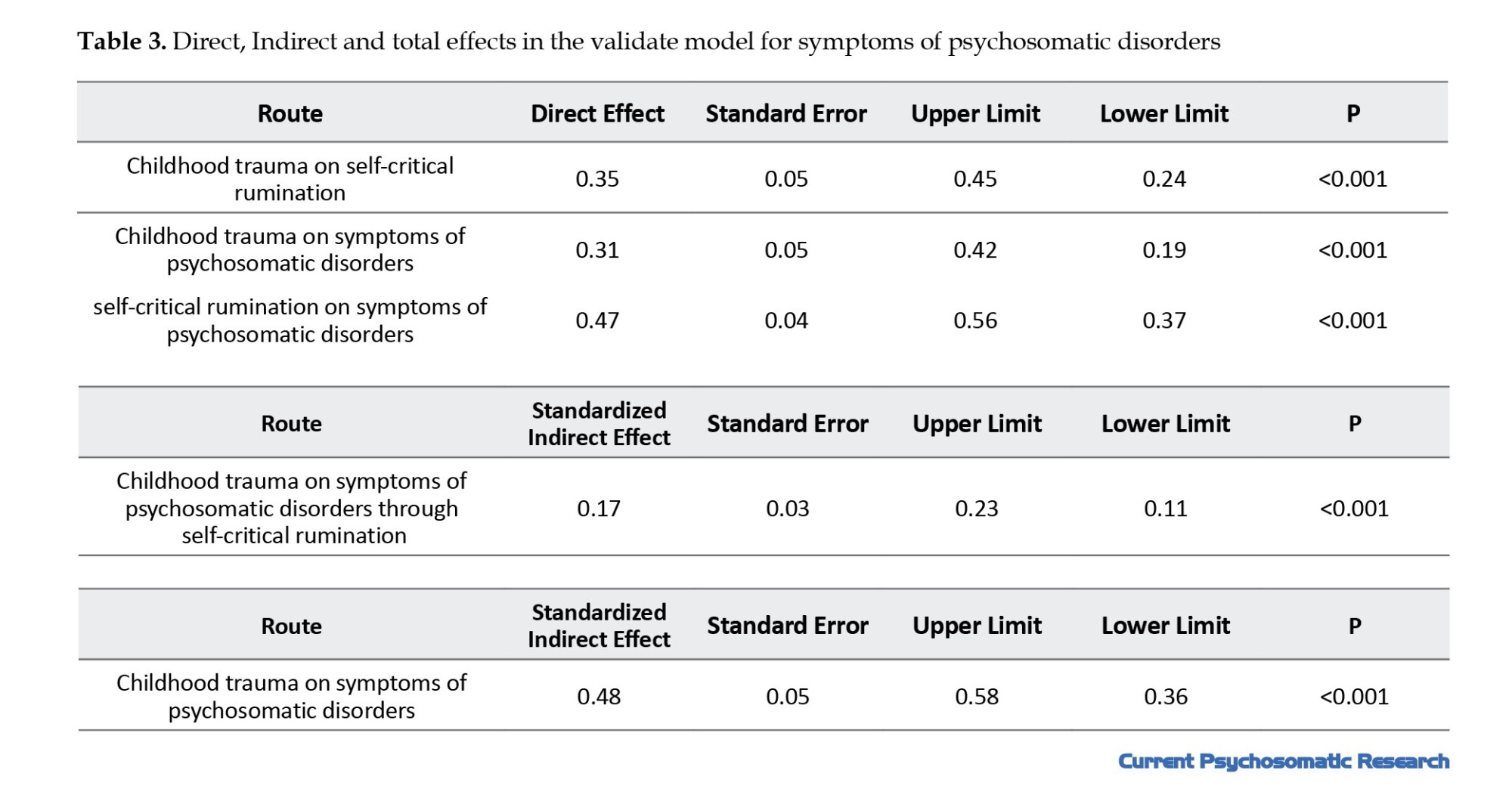
In Figure 1, the validated model for psychosomatic symptoms is shown. According to the fit indices (χ²/df=1.00, P=0.44 ,RMSEA=0.001, GFI=0.98, AGFI=0.97, CFI=1.00, SRMR=0.03, NFI=0.98), the model demonstrates a “good” fit. Based on this model, childhood trauma has a direct positive effect on self-critical rumination (t=6.05, P<0.001) and on psychosomatic symptoms (t=6.13, P<0.001). Additionally, self-critical rumination has a direct positive effect on psychosomatic symptoms (t=9.95, P<0.001).
According to the results presented in Table 3, the exogenous variable childhood trauma had a significant and positive indirect effect on the endogenous variable—psychosomatic symptoms through the mediating variable of self-critical rumination (β=0.17, P<0.001). In other words, the mediator variable, self-critical rumination, significantly mediated the relationship between childhood trauma and psychosomatic symptoms.
Furthermore, the R² index indicates the proportion of variance explained in the endogenous variable [47]. R² values of 0.26, 0.13, and 0.02 are described as strong, moderate, and weak, respectively. In the validated model, the coefficient of determination (R²) for psychosomatic symptoms was 0.43, indicating that the exogenous and mediating variables childhood trauma and self-critical rumination together explained 43% of the variance in psychosomatic symptoms. This level of explained variance is considered strong.
Discussion
The research question was as follows: Does self-critical rumination significantly mediate the relationship between childhood trauma and psychosomatic symptoms?
To address this question, a conceptual model was developed Figure 2, and its fit was examined using path analysis.
The findings of this study showed that childhood trauma had a significant and positive indirect effect on psychosomatic symptoms through the mediating variable of self-critical rumination. In other words, self-critical rumination played a significant mediating role in the relationship between childhood trauma and psychosomatic symptoms. Childhood trauma and the resulting psychological wounds have a profound impact on children’s health and development, often leading to both short- and long-term emotional and behavioral problems, and potentially resulting in psychiatric or medical disorders [48].
The more severe and widespread the childhood trauma, the greater the likelihood and intensity of psychosomatic symptoms [49]. Experiences of physical neglect may contribute to the development and maintenance of psychosomatic disorders through psychological mechanisms, such as difficulties in identifying and expressing emotions (alexithymia) [50] Several studies have also shown that emotional neglect leads to an inability to express and process emotions. This increases chronic stress in the individual, which keeps the autonomic and central hypothalamic-pituitary-adrenal (HPA) systems active. This repeated activation can cause traumatic reactions and physical disorders that ultimately manifest themselves in the form of psychosomatic symptoms [51]. Emotional abuse increases rumination, self-criticism, and emotional dysregulation, which increase psychological stress and lead to the emergence or exacerbation of psychosomatic symptoms [52]. Individuals with such trauma often attempt to keep themselves constantly busy in order to avoid confronting their stress. They may mistakenly believe that these avoidance strategies have eliminated their stress, while in reality, the stress remains repressed and denied, manifesting through ruminative thoughts. This unprocessed stress is discharged in maladaptive bodily forms, intensifying physical symptoms [53]. The internal psychological processes stemming from early abuse or neglect can lead to excessive self-criticism and rumination [32]. Rumination, especially in people who are emotionally abused, increases stress and anxiety. Emotional abuse predisposes to the formation of ruminative thought patterns that are accompanied by intense self-criticism [54]. Childhood trauma predisposes individuals to self-critical rumination, which in turn contributes to the development of psychosomatic disorders [28]. Many individuals suffering from psychosomatic symptoms have experienced physical or sexual abuse in the context of dysfunctional parenting, disrupted attachments, neglect, and emotional rejection. Those whose emotional needs were consistently overlooked may come to believe that the only way to gain attention or care is through physical discomfort [53].
Patients with traumatic experiences tend to express more intense emotions. Techniques such as hypnosis and emotional catharsis through revisiting traumatic memories may help alleviate physical symptoms. According to psychoanalytic findings, if trauma remains unresolved, it will persist somatically and eventually contribute to physical illness [22].
The roots of self-critical rumination can often be traced back to childhood, especially when caregivers frequently criticized the child. In such cases, the child may internalize negative thoughts and continue the cycle of self-critical rumination. Children subjected to intense parental criticism are more likely to continue the pattern of self-criticism in adulthood. The criticized child may, in essence, become their own aggressor [54].
The experience of childhood trauma can affect mental health by fostering self-critical rumination, which may function as a coping mechanism in the context of early adversity. Therefore, it can be expected that childhood trauma, in addition to its direct effect, may also have an indirect effect on psychosomatic symptoms through self-critical rumination [55]. The present study included a relatively homogeneous sample in terms of gender and age, with most participants being young women (18–25 years old). This demographic composition may impose limitations on the interpretation and generalizability of the findings. Research has shown that the experience and reporting of childhood trauma [56], the level of self-critical rumination [57], and the manifestation of psychosomatic symptoms [58] may vary according to factors such as gender and age. Specifically, women tend to report more psychosomatic symptoms and higher levels of rumination than men [59], and they may also be more vulnerable to the long-term effects of childhood trauma. Therefore, the findings of this study should be interpreted with caution, and future research should include samples with greater diversity in age and gender
Like other studies, the present research had limitations in its design and implementation:
1) This study used self-report instruments and a non-clinical sample, which necessitates caution when generalizing the findings to clinical populations. 2) In the CTQ, participants may not have recalled or reconstructed their past experiences accurately, possibly affecting the precision of the data. 3) Non-random (convenience) sampling through social networks may lead to selection bias; for example, individuals with more severe symptoms, such as anxiety, may be more attracted to the questionnaire, or those with access to the internet and smartphones may be more likely to participate.
Based on the findings of this study and the significant impact of childhood trauma on psychosomatic symptoms, it is recommended that physicians refer patients exhibiting such symptoms to psychologists. This allows for psychological intervention alongside medical treatment, thereby improving the overall physical and mental condition of the patient. Furthermore, healthcare and psychological counseling centers can utilize these findings to enhance prevention and treatment programs for childhood trauma and psychosomatic disorders.
Conclusion
The results of this study indicated that childhood trauma has both direct and indirect associations with psychosomatic symptoms in adulthood, with self-critical rumination playing a significant mediating role in this relationship. Traumatic experiences in childhood can activate maladaptive psychological processes, such as self-criticism and persistent ruminative thinking about the trauma, which ultimately exacerbate physical symptoms. These findings highlight the importance of identifying psychological mediating pathways between childhood trauma and somatic health and suggest that targeted interventions aimed at reducing self-critical rumination and enhancing coping skills may play a crucial role in preventing or alleviating psychosomatic problems.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Khayyam University, Mashhad, Iran (Code: IR.KHAYYAM.REC.1404.004).
Funding
This article is extracted from the master’s thesis of Mohadese Yazdani, approved by Khayyam University, Mashhad, Iran.
Authors' contributions
Conceptualization and supervision: Fatemeh AliDoosti; Methodology: Fatemeh AliDoosti and Mohadese Yazdani; Original draft writing: Mohadese Yazdani; Review and editing: Fatemeh AliDoosti; Data collection: Mohadese Yazdani; Data analysis: All authors.
Conflict of interest
The authors declared no conflict of interest
Acknowledgments
The authors sincerely acknowledge the faculty members and colleagues of the Department of Psychology at Khayyam University for their guidance, supervision, and scientific support throughout this study. The authors also sincerely thank all participants for their time and cooperation in this research.
References
In recent decades, a new category of illnesses known as psychosomatic disorders has emerged, in which emotional and psychological factors play a significant role in their development. According to the diagnostic and statistical manual of mental disorders [1], psychosomatic disorders encompass a broad range of conditions where physical symptoms constitute the core component [2]. As one of the common psychiatric disorders, psychosomatic illness represents a critical issue concerning both physical and mental health. These conditions often respond poorly to both pharmacological treatments and psychotherapy, resulting in substantial direct and indirect costs [3].
The term psychosomatic disorder is used when an individual presents with physical symptoms that appear to be primarily caused or exacerbated by psychological factors, without sufficient medical explanations. These symptoms often coexist with common medical and psychological issues, where psychological and somatic elements are intricately intertwined [4].
Psychiatric comorbidities are highly prevalent in such patients, with reported prevalence rates ranging from 20% to 67%, depending on the specific illness. Global studies indicate that the prevalence of psychosomatic disorders varies and is influenced by gender, cultural background, ethnicity, and various socio-economic factors [5]. Research conducted in European countries has shown that the prevalence of psychosomatic disorders is 18% in Denmark [6]. 70% among youth, 78% among middle-aged individuals, and 81% among the elderly in the Netherlands, and 22% in the United Kingdom [7].
Psychosomatic symptoms may reflect unresolved psychological pain or traumatic life experiences, significant losses, deep personal injuries, or experiences of dehumanization [8]. Some victims of physical violence report severe physical complaints and illnesses. Overall, many object relations theorists consider early developmental trauma as the root of psychosomatic disorders [9]. Children who experience parental abuse are at greater risk of developing various psychiatric problems, including depression, anxiety, psychosis, and personality disorders [10]. Indeed, trauma is one of the key factors that can trigger psychosomatic symptoms in individuals. Childhood maltreatment significantly undermines a child’s well-being and its effects often extend into adulthood [11].
adverse childhood experiences (ACEs) or childhood trauma refer to critical or deep-rooted events that threaten a child’s physical or emotional well-being. The term was first introduced in the study by Ferrari et al. [12] and encompasses a wide range of abusive experiences, including physical abuse, sexual abuse, emotional abuse, as well as neglect, such as physical and emotional neglect. It also includes experiences such as family dysfunction, lack of emotional and educational support, being raised by a family member with a mental illness, parental divorce, or domestic violence [13].
Childhood trauma involves any action or omission by parents or caregivers that causes harm—either overt or covert—or places the child at risk of harm, even if the intent was not to inflict harm [14]. Such experiences may leave the individual feeling vulnerable emotionally, cognitively, and physically, and can adversely affect multiple domains of development, including neurobiological, cognitive, emotional, and general health [15, 16].
Maltreatment causes stress that interferes with early brain development and can disrupt the growth of both the nervous and immune systems. As a result, children who experience maltreatment are at increased risk for behavioral problems, physical health issues, and mental health challenges. In the absence of emotional awareness, these children may indirectly exhibit symptoms of internalizing disorders. Such disorders may manifest as failure to gain expected weight, insomnia or hypersomnia, feelings of worthlessness or excessive guilt, reduced ability to think or concentrate, and recurrent thoughts of death—all of which may overlap with psychosomatic symptoms [17].
Numerous studies have demonstrated a link between childhood trauma and various psychological and physical disorders in adulthood. For instance, Kamandloo et al. [18] found that beyond the widespread cultural emphasis on attractiveness, past trauma and intrapsychic concerns may increase individuals’ sensitivity to rejection and preoccupation with physical appearance. Doba et al. [19] reported that experiencing negative emotions and emotional neglect by caregivers during childhood is associated with alexithymia and increased social isolation in adulthood. Furthermore, physical and emotional abuse in childhood predicts a greater tendency toward self-harming behaviors, aggression, and a reduced capacity for empathy, particularly in intimate relationships in later life [20].
According to the psychosomatic inhibition perspective, the inhibition of thoughts, feelings, or behaviors is accompanied by physiological activity. In the short term, inhibition leads to increased activity of the autonomic nervous system. Over time, inhibition acts as a cumulative stressor that increases the likelihood of developing psychosomatic illnesses.
Actively avoiding thinking or feeling about a trauma, or not talking about it, is considered a particularly harmful form of inhibition. Findings from recent surveys and experiments indicate that childhood traumatic experiences—especially those never discussed—are strongly associated with current physical health problems; recent traumas that have not been discussed are linked to increased physical problems and rumination about the traumas; confronting earlier traumas through writing improves health and immune system functioning; actively talking about distressing experiences is associated with immediate reductions in certain autonomic nervous system activities [21].
One common coping mechanism individuals may adopt in response to traumatic experiences is rumination [22]. There is a significant relationship between childhood trauma and increased levels of rumination in adulthood [23]. Rumination refers to a persistent tendency to think repeatedly about the causes and consequences of negative emotional experiences [24]. Individuals who engage in rumination are more likely to dwell on negative memories, interpret events pessimistically, and, consequently, experience lower life satisfaction and a more negative outlook on life [25].
Rumination exists in various forms, one of which is self-critical rumination. This involves persistent negative self-evaluation, characterized by self-deprecating, judgmental, or pessimistic thoughts related to failures, disappointments, or unattained goals [26]. In this form of rumination, the individual often focuses on perceived worthlessness, shameful aspects of the self, or guilt-inducing thoughts [27, 28]. In general, self-critical individuals tend to believe they have failed in life [29].
Self-critical rumination was a key finding in the study by Sen and Gumus [30], which explained how childhood maltreatment may impair psychological well-being in adulthood. Some studies have also shown that when self-criticism and rumination are combined, self-criticism becomes an even more serious threat to mental well-being [27]. Notably, self-critical rumination significantly predicts self-esteem, even when controlling for age, baseline self-criticism, anxiety, stress, and depression [31]. Persistent and excessive self-criticism, particularly in the form of self-critical rumination, may severely affect an individual’s self-concept, subjective well-being, and overall mental health outcomes [32].
Numerous studies have examined the mediating role of rumination in the relationship between childhood trauma and mental disorders, including study [33], which introduced the response style theory of depression. According to this theory, rumination is an important vulnerability factor for depression that can intensify and prolong depressive episodes [34]. Study also found that a ruminative response style can predict the severity of depression in both clinical and non-clinical samples after one year.
Rumination may contribute to depression by processing and reproducing traumatic childhood experiences. In general, recurring negative thoughts play a significant role in mood disorders and anxiety following a traumatic experience [35]. Another study showed that neuroticism is associated with self-criticism and a general tendency to evaluate oneself negatively. Neuroticism, also known as negative emotionality, is characterized by high sensitivity to negative emotions such as anxiety, anger, and depression, making individuals prone to interpreting events negatively [36].
Longitudinal studies have shown that self-critical rumination predicts future psychopathology (i.e. depressive symptoms, anxiety, or suicidal ideation) [37, 38]. When individuals engage in self-critical rumination, they become trapped in repetitive and persistent thinking about their distress, which can intensify emotional responses (i.e. psychopathology) [28].
Another finding indicated that forgiveness significantly mediates the relationship between childhood trauma and both rumination and intolerance of uncertainty, which in turn significantly mediates the relationship between childhood trauma and social anxiety. Moreover, indirect effects were observed through a sequential pathway from childhood trauma to forgiveness, then to rumination and intolerance of uncertainty, and finally to social anxiety [39].
In another study, it was reported that social stigma directly affects suicidal thoughts and indirectly influences them through deliberate rumination, which mediates 92% of the total effect. These findings suggest that deliberate rumination functions as a cognitive reappraisal mechanism that disrupts the social stigma–suicidality pathway, aligning with the cognitive-behavioral theory’s focus on restructuring maladaptive schemas [40].
But, childhood trauma and maltreatment are among the factors that may contribute to psychosomatic symptoms. Furthermore, childhood trauma may influence the development of such symptoms through mediating variables, such as self-critical rumination. Given the complexity and lack of clarity surrounding the mechanisms and manifestations of psychosomatic disorders, conducting research that seeks to identify and clarify their connections to ACEs and self-critical rumination is of significant importance. Therefore, the present study aims to investigate the following research question: Does self-critical rumination mediate the relationship between childhood trauma and psychosomatic symptoms?
Materials and Methods
This study employed a fundamental research design in terms of purpose and was correlational in terms of data collection, specifically using Path analysis. The statistical population consisted of all adults over 18 years of age in Razavi Khorasan Province between March 2024 and June 2024. According to Schumacher and Lomax’s recommendations for Modeling studies, a sample size between 200 and 600 participants is considered sufficient. Accordingly [41], 300 participants were selected for the current study.
The questionnaires were administered online via the “Porsline” platform and distributed through social media. The inclusion criterion for participants was an age range between 18 and 50 years. Ethical considerations were strictly observed. Along with the questionnaire link, participants received a brief explanation outlining the study’s purpose, assurance of anonymity and confidentiality, and the voluntary nature of participation. Participants were asked to complete the questionnaire only after providing informed consent.
Demographic questionnaire
This section includes questions about gender, age, marital status, employment status, and education.
Childhood trauma questionnaire (CTQ)
Developed by Bernstein et al. [42], the CTQ is suitable for both adults and adolescents. It assesses five types of childhood maltreatment: sexual abuse, physical abuse, emotional abuse, physical neglect, and emotional neglect. The CTQ contains 28 items, of which 25 measure core components and 3 are validity items for identifying individuals who may minimize or deny their traumatic experiences. Higher scores indicate greater levels of trauma. Each subscale ranges from 5 to 25, and the total score ranges from 25 to 125. Previous research reported Cronbach’s α ranging from 0.86 to 0.95 for subscales and construct validity between 0.59 and 0.78. Specifically, the emotional abuse and emotional neglect subscales demonstrated alphas of 0.86 and 0.89, respectively [43]. In this study, the validity of the childhood trauma scale using Cronbach’s α coefficient method was 0.86 for the entire scale and 0.88 for the sexual abuse components, 0.79 for the physical abuse components, 0.81 for the emotional abuse components, 0.86 for the emotional neglect components, and 0.72 for the physical neglect components.
Psychosomatic symptoms questionnaire
Validated by Takata and Sakata [44], this questionnaire consists of 30 items, each rated on a 4-point Likert scale: Never (0), rarely (1), sometimes (2), and frequently (3). The total score ranges from 0 to 90. The authors reported Cronbach’s α between 0.90 and 0.93 across three administrations. Concurrent validity was confirmed through correlation with the Goldberg general health questionnaire, yielding coefficients of 0.64 and 0.65. Construct validity was assessed using factor analysis, with Cronbach’s α values of 0.93 and 0.92. Test-re-test correlations exceeded r=0.5 across three measurements [44]. In this study, the validity of the psychosomatic disorders scale was 0.93.
Self-critical rumination scale (SCRS)
Developed by Smart et al. [27], the SCRS includes 10 items. Items with skewness exceeding three times the standard error were retained due to content importance. Items were derived from both clinical and student samples, as well as existing rumination criteria. The scale uses a 4-point Likert format ranging from 1 (Not at all) to 4 (Very much), with higher scores reflecting greater levels of self-critical rumination. Fearn et al. [28] reported a Cronbach’s α of 0.91, indicating excellent internal consistency. In this study, the validity of the SCRS was 0.90. The collected data were analyzed using SPSS software, version 26 and AMOS software, version 24 at two levels:
Descriptive statistics: Frequency, percentage, Mean±SD. Inferential statistics: Pearson correlation and Path analysis. To examine the normality of the data, according to Chu and Bentler [45], skewness values within ±3 and, based on Kline [46], kurtosis values within ±10 are considered acceptable. In the present study, skewness values (0.20–2.88) and kurtosis values (0.03–9.39) for childhood trauma scores, self-critical rumination, and psychosomatic symptoms were within the acceptable range; therefore, it can be concluded that the data for these variables were normally distributed. In addition, to assess multicollinearity, the variance inflation factor (VIF) and tolerance indices were used. The results indicated that VIF values (1.13–2.75) were below 10, and tolerance values (0.36–0.88) were within the 0–1 range. Thus, it can be stated that no multicollinearity existed among the predictor variables. Furthermore, to ensure that the assumptions of the model were met, the independence of errors was examined using the Durbin–Watson statistic. The obtained value (1.95) for predicting psychosomatic symptoms was less than 4; therefore, it can be concluded that autocorrelation was absent and the assumption of error independence was satisfied.
Results
In this study, the majority of participants were female (84.3%), aged 18–25 years (49.7%), held a bachelor’s degree (42.7%), were married (41.7%), and were unemployed (45.7%). Descriptive statistics, including Mean±SD for childhood trauma, self-critical rumination, and psychosomatic symptoms, are presented in Table 1. The mean scores for total childhood trauma, self-critical rumination, and psychosomatic symptoms were 39.93±13.83, 24.22±7.49, and 34.27±16.62, respectively.
Initially, in order to examine the relationship between demographic variables and trauma, the results of the t-test to compare women and men in the trauma score (t=0.52, P=0.598), as well as, the results of the ANOVA test to compare different age groups (F=1.93, P=0.124) and different educational levels (F=0.59, P=0.669) in the scores of this variable were examined, and all of these results indicated no significant difference.
According to the Pearson correlation coefficients presented in Table 2, childhood trauma and all of its components showed a significant positive correlation with psychosomatic symptoms and self-critical rumination.
The positive direction of these correlations indicates that higher levels of childhood trauma and its subcomponents were associated with higher levels of psychosomatic symptoms and self-critical rumination among the study participants.
According to this model, childhood trauma was considered as the exogenous latent variable (with observed subcomponents), self-critical rumination served as the mediator, and psychosomatic symptoms were treated as the endogenous variable, with both the mediator and outcome variables being observed variables.
Model fit was evaluated through path analysis using indices such as chi-square (χ²), comparative fit index (CFI), goodness of fit index (GFI), adjusted goodness of fit index (AGFI), and the root mean square error of approximation (RMSEA). For acceptable model fit, the standard criteria are as follows: A chi-square to degrees of freedom ratio (χ²/df) less than 3; CFI, GFI, and AGFI values close to 1; and RMSEA between 0 and 0.05 (indicating a good fit), or between 0.05 and 0.10 (indicating an acceptable fit). Although the chi-square index is commonly used to assess model fit, it tends to increase with larger sample sizes and degrees of freedom; therefore, the RMSEA is recommended as a more robust measure.
Based on these criteria, the overall model fit indices for the initial model were examined. The results indicated a “good” model fit, and the detailed findings are presented below.
In Figure 1, the validated model for psychosomatic symptoms is shown. According to the fit indices (χ²/df=1.00, P=0.44 ,RMSEA=0.001, GFI=0.98, AGFI=0.97, CFI=1.00, SRMR=0.03, NFI=0.98), the model demonstrates a “good” fit. Based on this model, childhood trauma has a direct positive effect on self-critical rumination (t=6.05, P<0.001) and on psychosomatic symptoms (t=6.13, P<0.001). Additionally, self-critical rumination has a direct positive effect on psychosomatic symptoms (t=9.95, P<0.001).
According to the results presented in Table 3, the exogenous variable childhood trauma had a significant and positive indirect effect on the endogenous variable—psychosomatic symptoms through the mediating variable of self-critical rumination (β=0.17, P<0.001). In other words, the mediator variable, self-critical rumination, significantly mediated the relationship between childhood trauma and psychosomatic symptoms.
Furthermore, the R² index indicates the proportion of variance explained in the endogenous variable [47]. R² values of 0.26, 0.13, and 0.02 are described as strong, moderate, and weak, respectively. In the validated model, the coefficient of determination (R²) for psychosomatic symptoms was 0.43, indicating that the exogenous and mediating variables childhood trauma and self-critical rumination together explained 43% of the variance in psychosomatic symptoms. This level of explained variance is considered strong.
Discussion
The research question was as follows: Does self-critical rumination significantly mediate the relationship between childhood trauma and psychosomatic symptoms?
To address this question, a conceptual model was developed Figure 2, and its fit was examined using path analysis.
The findings of this study showed that childhood trauma had a significant and positive indirect effect on psychosomatic symptoms through the mediating variable of self-critical rumination. In other words, self-critical rumination played a significant mediating role in the relationship between childhood trauma and psychosomatic symptoms. Childhood trauma and the resulting psychological wounds have a profound impact on children’s health and development, often leading to both short- and long-term emotional and behavioral problems, and potentially resulting in psychiatric or medical disorders [48].
The more severe and widespread the childhood trauma, the greater the likelihood and intensity of psychosomatic symptoms [49]. Experiences of physical neglect may contribute to the development and maintenance of psychosomatic disorders through psychological mechanisms, such as difficulties in identifying and expressing emotions (alexithymia) [50] Several studies have also shown that emotional neglect leads to an inability to express and process emotions. This increases chronic stress in the individual, which keeps the autonomic and central hypothalamic-pituitary-adrenal (HPA) systems active. This repeated activation can cause traumatic reactions and physical disorders that ultimately manifest themselves in the form of psychosomatic symptoms [51]. Emotional abuse increases rumination, self-criticism, and emotional dysregulation, which increase psychological stress and lead to the emergence or exacerbation of psychosomatic symptoms [52]. Individuals with such trauma often attempt to keep themselves constantly busy in order to avoid confronting their stress. They may mistakenly believe that these avoidance strategies have eliminated their stress, while in reality, the stress remains repressed and denied, manifesting through ruminative thoughts. This unprocessed stress is discharged in maladaptive bodily forms, intensifying physical symptoms [53]. The internal psychological processes stemming from early abuse or neglect can lead to excessive self-criticism and rumination [32]. Rumination, especially in people who are emotionally abused, increases stress and anxiety. Emotional abuse predisposes to the formation of ruminative thought patterns that are accompanied by intense self-criticism [54]. Childhood trauma predisposes individuals to self-critical rumination, which in turn contributes to the development of psychosomatic disorders [28]. Many individuals suffering from psychosomatic symptoms have experienced physical or sexual abuse in the context of dysfunctional parenting, disrupted attachments, neglect, and emotional rejection. Those whose emotional needs were consistently overlooked may come to believe that the only way to gain attention or care is through physical discomfort [53].
Patients with traumatic experiences tend to express more intense emotions. Techniques such as hypnosis and emotional catharsis through revisiting traumatic memories may help alleviate physical symptoms. According to psychoanalytic findings, if trauma remains unresolved, it will persist somatically and eventually contribute to physical illness [22].
The roots of self-critical rumination can often be traced back to childhood, especially when caregivers frequently criticized the child. In such cases, the child may internalize negative thoughts and continue the cycle of self-critical rumination. Children subjected to intense parental criticism are more likely to continue the pattern of self-criticism in adulthood. The criticized child may, in essence, become their own aggressor [54].
The experience of childhood trauma can affect mental health by fostering self-critical rumination, which may function as a coping mechanism in the context of early adversity. Therefore, it can be expected that childhood trauma, in addition to its direct effect, may also have an indirect effect on psychosomatic symptoms through self-critical rumination [55]. The present study included a relatively homogeneous sample in terms of gender and age, with most participants being young women (18–25 years old). This demographic composition may impose limitations on the interpretation and generalizability of the findings. Research has shown that the experience and reporting of childhood trauma [56], the level of self-critical rumination [57], and the manifestation of psychosomatic symptoms [58] may vary according to factors such as gender and age. Specifically, women tend to report more psychosomatic symptoms and higher levels of rumination than men [59], and they may also be more vulnerable to the long-term effects of childhood trauma. Therefore, the findings of this study should be interpreted with caution, and future research should include samples with greater diversity in age and gender
Like other studies, the present research had limitations in its design and implementation:
1) This study used self-report instruments and a non-clinical sample, which necessitates caution when generalizing the findings to clinical populations. 2) In the CTQ, participants may not have recalled or reconstructed their past experiences accurately, possibly affecting the precision of the data. 3) Non-random (convenience) sampling through social networks may lead to selection bias; for example, individuals with more severe symptoms, such as anxiety, may be more attracted to the questionnaire, or those with access to the internet and smartphones may be more likely to participate.
Based on the findings of this study and the significant impact of childhood trauma on psychosomatic symptoms, it is recommended that physicians refer patients exhibiting such symptoms to psychologists. This allows for psychological intervention alongside medical treatment, thereby improving the overall physical and mental condition of the patient. Furthermore, healthcare and psychological counseling centers can utilize these findings to enhance prevention and treatment programs for childhood trauma and psychosomatic disorders.
Conclusion
The results of this study indicated that childhood trauma has both direct and indirect associations with psychosomatic symptoms in adulthood, with self-critical rumination playing a significant mediating role in this relationship. Traumatic experiences in childhood can activate maladaptive psychological processes, such as self-criticism and persistent ruminative thinking about the trauma, which ultimately exacerbate physical symptoms. These findings highlight the importance of identifying psychological mediating pathways between childhood trauma and somatic health and suggest that targeted interventions aimed at reducing self-critical rumination and enhancing coping skills may play a crucial role in preventing or alleviating psychosomatic problems.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Khayyam University, Mashhad, Iran (Code: IR.KHAYYAM.REC.1404.004).
Funding
This article is extracted from the master’s thesis of Mohadese Yazdani, approved by Khayyam University, Mashhad, Iran.
Authors' contributions
Conceptualization and supervision: Fatemeh AliDoosti; Methodology: Fatemeh AliDoosti and Mohadese Yazdani; Original draft writing: Mohadese Yazdani; Review and editing: Fatemeh AliDoosti; Data collection: Mohadese Yazdani; Data analysis: All authors.
Conflict of interest
The authors declared no conflict of interest
Acknowledgments
The authors sincerely acknowledge the faculty members and colleagues of the Department of Psychology at Khayyam University for their guidance, supervision, and scientific support throughout this study. The authors also sincerely thank all participants for their time and cooperation in this research.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders DSM-5. 5rd ed [F. Gholamian, S. S. Mousavi, A. Mohamadsadegh, Persian trans.]. Tehran: Arjmand Publications; 2021. [Link]
- Ower C, Kemmler G, Vill T, Martini C, Schmitt A, Sperner-Unterweger B, et al. The effect of physical activity in an alpine environment on quality of life is mediated by resilience in patients with psychosomatic disorders and healthy controls. Eur Arch Psychiatry Clin Neurosci. 2019; 269(5):543-53. [DOI:10.1007/s00406-018-0930-2] [PMID]
- Okur Güney ZE, Sattel H, Witthöft M, Henningsen P. Emotion regulation in patients with somatic symptom and related disorders: A systematic review. Plos One. 2019; 14(6):e0217277. [DOI:10.1371/journal.pone.0217277] [PMID]
- Farzadfar F, Naghavi M, Sepanlou SG, Moghaddam SS, Dangel WJ, Weaver ND, et al. Health system performance in Iran: A systematic analysis for the global burden of disease study 2019. Lancet. 2022; 399(10335):1625-45. [Link]
- Khodayari Fard M, Abedini Y. [Cognitive behavioral family therapy in the treatment of patients with musculoskeletal pain (Persian)]. Dev Psychol. 2006; 2(8):277-85. [Link]
- Perry JC, Presniak MD, Olson TR. Defense mechanisms in schizotypal, borderline, antisocial, and narcissistic personality disorders. Psychiatry. 2013; 76(1):32-52. [DOI:10.1521/psyc.2013.76.1.32] [PMID]
- Babaei S, Manesh MN, Abouzari F, Karami S. [The role of traumatic childhood experiences, mentalization and Alexithymia in predicting depression and suicidal thoughts in women suffering from the trauma of marital betrayal (Persian)]. Iran J Psychiatr Nurs. 2023; 10(6):110-22. [DOI:10.22034/IJPN.10.6.110]
- Cakmur H. Effects of Stress on Human Health. First Edition. Ankara: IntechOpen; 2020.
- Namjoo S, Nouri A. [The effectiveness of mindfulness-based cognitive therapy training on psychosomatic symptoms, self-dissociation, and attachment style of women with psychosomatic symptoms (Persian)]. J Psychol. 2023; 12(4):127-38. [Link]
- Lotzin A, Grundmann J, Hiller P, Pawils S, Schäfer I. Profiles of childhood trauma in women with substance use disorders and comorbid posttraumatic stress disorders. Front Psychiatr. 2019; 10:674. [DOI:10.3389/fpsyt.2019.00674] [PMID]
- Destree L, Brierley ME, Albertella L, Jobson L, Fontenelle LF. The effect of childhood trauma on the severity of obsessive-compulsive symptoms: A systematic review. J Psychiatry Res. 2021; 142:345-60. [DOI:10.1016/j.jpsychires.2021.08.017] [PMID]
- Ferrari A, Santomauro D, Ashbaugh C, Hay S, Vos T, Whiteford H. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatr. 2022; 9(2):137–50.
- Taşören AB, Gül İŞ. The role of childhood abuse and psychological symptoms in discriminating frequency of drug use and self-harm in incarcerated men convicted of robbery. Curr App Psychiatry. 2022; 14(Ek 1):83-91.[DOI:10.18863/pgy.1083683]
- Cohrdes C, Mauz E. Self-efficacy and emotional stability buffer negative effects of adverse childhood experiences on young adult health-related quality of life. J Adolesc Health. 2020; 67(1):93-100. [DOI:10.1016/j.jadohealth.2020.01.005] [PMID]
- Abraham EH, Antl SM, McAuley T. Trauma exposure and mental health in a community sample of children and youth. Psychol Trauma. 2022; 14(4):624-32. [DOI:10.1037/tra0001035] [PMID]
- Luoni C, Agosti M, Crugnola S, Rossi G, Termine C. Psychopathology, dissociation and somatic symptoms in adolescents who were exposed to traumatic experiences. Front Psychol. 2018; 9:2390. [DOI:10.3389/fpsyg.2018.02390] [PMID]
- Erfanifar F, Zarani F, Shokri O, Kabiri Agh Ziarat S. Child neglect and internalizing disorders: The mediating role of emotion regulation. J Child Ment Health. 2019; 6(1):112-23. [DOI:10.29252/jcmh.6.1.10]
- Kamandloo M, Karami S, Balashour B, Shahini M. [The relationship between childhood trauma experience with anxiety symptoms and body dysmorphic disorder in cosmetic surgery applicants with the mediation of rejection sensitivity (Persian)]. Iran J Psychiatr Nurs. 2024; 12(1):64-77. [DOI:10.22034/IJPN.12.1.64]
- Doba K, Saloppé X, Choukri F, Nandrino JL. Childhood trauma and posttraumatic stress symptoms in adolescents and young adults: The mediating role of mentalizing and emotion regulation strategies. Child Abuse Neglect. 2022; 132:105815. [DOI:10.1016/j.chiabu.2022.105815] [PMID]
- Barczyk ZA, Foulds JA, Porter RJ, Douglas KM. Childhood trauma and cognitive functioning in mood disorders: A systematic review. Bipolar Disord. 2023; 25(4):263-77. [DOI:10.1111/bdi.13321] [PMID]
- Pennebaker JW, Susman JR. Disclosure of traumas and psychosomatic processes. Soc Sci Med. 1988; 26(3):327-32. [DOI:10.1016/0277-9536(88)90397-8] [PMID]
- Thomsen DK, Mehlsen MM, Christensen S, Zachariae R. Rumination-relationship with negative mood and sleep quality. Pers Individ Diff. 2003; 34(7):1293-301. [DOI:10.1016/S0191-8869(02)00120-4]
- Brown VM, Morey RA. Neural systems for cognitive and emotional processing in posttraumatic stress disorder. Front Psychol. 2012; 3:449. [DOI:10.3389/fpsyg.2012.00449]
- Yadollahifar S, Sadeghi A, Shamsaei F. The relationship between rumination and sleep quality in patients with major depressive disorder. Shenakht J Psychol Psychiatry. 2020; 7(2):26-36. [DOI:10.52547/shenakht.7.2.26]
- Rowley AA, Roesch SC, Jurica BJ, Vaughn AA. Developing and validating a stress appraisal measure for minority adolescents. J Adolesce. 2005; 28(4):547-57. [DOI:10.1016/j.adolescence.2004.10.010] [PMID]
- Shahar G. Erosion: The psychopathology of self-criticism. 3rd. Oxford: Oxford University Press; 2015. [DOI:10.1093/med:psych/9780199929368.001.0001]
- Smart LM, Peters JR, Baer RA. Development and validation of a measure of self-critical rumination. Assessment. 2016; 23(3):321-32. [DOI:10.1177/1073191115573300] [PMID]
- Fearn M, Marino C, Spada MM, Kolubinski DC. Self-critical rumination and associated metacognitions as mediators of the relationship between perfectionism and self-esteem. J Ration Emot Cogn Behav Ther. 2022; 40(1):155-74. [DOI:10.1007/s10942-021-00404-4] [PMID]
- Stoner P. Vulnerable narcissism, self-criticism, and self-injurious behavior: 201 regulation as a moderator [master thesis]. Hattiesburg: University of Southern Mississippi; 2016. [Link]
- Cecen AR, Gümüş Z. The underlying mechanism for childhood psychological maltreatment and self-satisfaction: The serial mediating roles of self-critical rumination and self-compassion. Int J Ment Health Addict. 2025; 23(3):2252-68. [DOI:10.1007/s11469-023-01228-2]
- Kolubinski DC, Marino C, Nikčević AV, Spada MM. A metacognitive model of self-esteem. J Affect Disord. 2019; 256:42-53. [DOI:10.1016/j.jad.2019.05.050] [PMID]
- Collins S, Orth T, Brunton R, Dryer R. Child abuse and wellbeing: Examining the roles of self-compassion and fear of self. Child Abuse Negl. 2023; 138:106089. [DOI:10.1016/j.chiabu.2023.106089] [PMID]
- Nolen-Hoeksema S. Sex differences in unipolar depression: Evidence and theory. Psychol Bull. 1987; 101(2):259-82.[DOI:10.1037//0033-2909.101.2.259] [PMID]
- Nolen-Hoeksema S. The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J Abnorm Psychol. 2000; 109(3):504. [DOI:10.1037//0021-843X.109.3.504] [PMID]
- Squires SD, Hu M, Milev RV, Poppenk J. The impact of non-infection pandemic stress on depression and anxiety severity: Investigating mediation by intrusive and deliberate rumination. J Affect Disord. 2022; 310:291-5.[DOI:10.1016/j.jad.2022.05.039] [PMID]
- Widiger TA, Oltmanns JR. Neuroticism is a fundamental domain of personality with enormous public health implications. World Psychiatry. 2017 16(2):144. [DOI:10.1002/wps.20411] [PMID]
- Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin Psychol Rev. 2010; 30(2):217-37. [DOI:10.1016/j.cpr.2009.11.004] [PMID]
- Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking rumination. Perspectives on psychological science. 2008; 3(5):400-24. [DOI:10.1111/j.1745- 6924.2008.00088.x] [PMID]
- Uzun K, Arslan G. Adverse childhood experiences, forgiveness, rumination, intolerance of uncertainty, and social anxiety in emerging adults: A multi-mediation analysis. Psychol Rep. 2025; 332941251363472. [DOI:10.1177/00332941251363472] [PMID]
- Wang M, Kong Y, Chen Y, Lei Z, Lin Q, Zhou R, et al. How does deliberate rumination influence the association between stigma and suicide ideation in depressed patients: A mediation analysis. Int J Ment Health Nurs. 2025; 34(3):e70065. [DOI:10.1111/inm.70065] [PMID]
- Lomax RG, Schumacker RE. A beginner’s guide to structural equation modeling. 4th ed. New York: Routledge; 2016.[Link]
- Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, et al. Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse Neglect. 2003; 27(2):169-90. [DOI:10.1016/S0145-2134(02)00541-0] [PMID]
- Pourshahriar H, Alizadeh H, Rajai-nia K. [Childhood emotional abuse experience and borderline personality disorder characteristics in adulthood: The mediating role of attachment styles and emotional regulation (Persian)]. Iran J Psychiatry Clin Psychol. 2018; 24(2):153-62. [DOI:10.32598/ijpcp.24.2.148]
- Takata Y, Sakata Y. Development of a psychosomatic complaints scale for adolescents. Psychiatry Clin Neurosci. 2004; 58(1):3-7. [DOI:10.1111/j.1440-1819.2004.01184.x] [PMID]
- Chu K, Bentler PM. Evaluation of normality assumptions in structural equation modeling. Psychol Methods. 1995; 1(2):171-80. [Link]
- Kline RB. Principles and practice of structural equation modeling. 4th ed. New York: Guilford Press; 2023. [Link]
- Cohen J. Statistical power analysis. Current directions in Psychol Sci. 1992; 1(3):98-101. [DOI:10.1111/1467-8721.ep10768783]
- Stubenbort K, Cohen MM, Trybalski V. The effectiveness of an attachment-focused treatment model in a therapeutic preschool for abused children. Clin Soc Work J. 2010; 38(1):51-60. [DOI:10.1007/s10615-007-0107-3]
- Farokhzadian AA, Rezaei F, Sadeghi M. Mediating role of emotional schemas in the relationship between childhood traumas and generalized anxiety disorder. Clin Psychol Pers. 2020; 17(2):89-101. [DOI:10.22070/cpap.2020.2910]
- Eapen V, Crncec R. Tourette syndrome in children and adolescents: special considerations. J Psychosom Res. 2009; 67(6):525-32. [DOI:10.1016/j.jpsychores.2009.08.003] [PMID]
- Walentynowicz M, Raes F, Van Diest I, Van den Bergh O. The specificity of health-related autobiographical memories in patients with somatic symptom disorder. Psychosom Med. 2017; 79(1):43-9. [DOI:10.1097/PSY.0000000000000357] [PMID]
- Spinhoven P, van Hemert AM, Penninx BW. Childhood trauma and personality traits in adult patients with depressive and anxiety disorders: mediating effects of rumination and self-criticism. Psychol Med. 2010; 40(8):1367-78. [Link]
- Afshari A, Jondi Z. [The role of child's self-efficacy in the relationship between childhood traumatic events and psychosomatic complaints (Persian)]. J Psychol Stud. 2021; 17(2):139-62. [DOI:10.22051/psy.2021.34386.2375]
- Gilbert P, Clarke M, Hempel S, Miles JN, Irons C. Criticizing and reassuring oneself: An exploration of forms, styles and reasons in female students. Br J Clin Psychol. 2004; 43(Pt 1):31-50. [DOI:10.1348/014466504772812959] [PMID]
- Rsalandeh F, Iliyaifar G, Shakibaeinezhad A, Ghanbari E. [The effect of childhood trauma and emotional dysregulation on suicidal thoughts with the mediation of rumination in nurses with depressive symptoms (Persian)]. J Nurs Manag. 2022; 12(3):90-104. [Link]
- Finkelhor D, Ormrod R, Turner H, Hamby SL. The victimization of children and youth: A comprehensive, national survey. Child Maltreat. 2005; 10(1):5-25.[DOI:10.1177/1077559504271287] [PMID]
- Rice KG, Leever BA, Noggle CA, Lapsley DK. Perfectionism and depressive symptoms in early adolescence. Psychol Sch. 2007; 44(2):139-56. [DOI:10.1002/pits.20212]
- Kirmayer LJ, Young A. Culture and somatization: Clinical, epidemiological, and ethnographic perspectives. Psychosom Med. 1998; 60(4):420-30. [DOI:10.1097/00006842-199807000-00006] [PMID]
- Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. J Abnorm Psychol. 1991; 100(4):569. [DOI:10.1037/0021-843X.100.4.569] [PMID]
Type of Study: Research |
Subject:
Psychology
Received: 2024/08/5 | Accepted: 2024/09/10 | Published: 2024/10/1
Received: 2024/08/5 | Accepted: 2024/09/10 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
