Wed, May 27, 2026
[Archive]
Volume 3, Issue 1 (Autumn 2024)
CPR 2024, 3(1): 15-24 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mousavi S, Fendereski A, Ghasemi F, Shafipour L, Bagherzadeh M, Shafipour V. Nurses’ Perceptions of the Quality of Nursing Care in Patients With COVID-19: A Cross-sectional Study. CPR 2024; 3 (1) :15-24
URL: http://cpr.mazums.ac.ir/article-1-146-en.html
URL: http://cpr.mazums.ac.ir/article-1-146-en.html
Sahba Mousavi 

 , Afsaneh Fendereski , Fahimeh Ghasemi , Leila Shafipour , Mahboobeh Bagherzadeh , Vida Shafipour
, Afsaneh Fendereski , Fahimeh Ghasemi , Leila Shafipour , Mahboobeh Bagherzadeh , Vida Shafipour
, Afsaneh Fendereski , Fahimeh Ghasemi , Leila Shafipour , Mahboobeh Bagherzadeh , Vida Shafipour
Department of Medical Surgical Nursing, Cardiovascular research center, Faculty of Nursing and Midwifery, Mazandaran University of Medical Sciences, Sari, Iran.
Full-Text [PDF 832 kb]
(36 Downloads)
| Abstract (HTML) (104 Views)
Full-Text: (20 Views)
Introduction
Ensuring and enhancing the quality of nursing care stands as a critical and ongoing challenge for healthcare systems globally, demanding continuous commitment and innovation to meet the evolving needs of patients [1]. The nurses’ professional expertise and experience are critical predictors of high-quality care [2]. Nurses are the primary agents of care quality; therefore, their perception of care quality should be taken seriously. Emerging studies have shown that both job satisfaction and nurses’ intention to leave the profession influence their perceptions of care quality [3]. Nurses may consider leaving their positions to seek more favorable environments when they perceive that their current working conditions fail to support professional standards [4]. Nurses’ insights into care quality and improvement strategies evolve through ongoing bedside practice. These perceptions reliably indicate actual care delivered. Assessing care quality via nurses’ views thereby evaluates treatment success and patient care standards [5].
During times of crisis, it is essential to understand how changes in providing healthcare impact healthcare professionals. As COVID-19, the acute respiratory syndrome, has fluctuated across countries, medical resources have remained uncertain, and healthcare priorities, policies and procedures have rapidly changed [6]. Because of the pandemic, nurses in hospital environments frequently worked extended hours and managed exceptionally high patient volumes, with limited chances for rest or recuperation [7]. In addition to facing these challenges, healthcare providers often struggle to balance their responsibilities toward patients, their families, and themselves. This dynamic, stressful, and uncertain environment can lead to situations where ethical values or obligations are compromised [6]. Healthcare workers may face situations where external factors like resource constraints, new health policies, or care models prevent them from acting in line with their core ethical beliefs. They often recognize ethical conflicts but feel powerless to maintain ethical standards due to these pressures. This results in a compromise of their professional integrity [8]. When such circumstances are repeated frequently, they can result in “moral injury”, exacerbating emotional distress, burnout, and frustration, and ultimately leading to workforce attrition [9].
Since the onset of COVID-19 in 2019, a major transformation has occurred in providing healthcare for professionals working in this field, significantly altering routine care practices [10, 11]. The intense workload in high-risk environments has even affected nursing care for non-COVID-19 patients [12, 13]. Healthcare workers have played a vital role in facilitating these changes and reported a wide range of experiences [14, 15]. Investigations into the care of patients with COVID-19 have highlighted the challenges in this area. Research conducted in Iran has shown that nurses caring for COVID-19 patients experience issues such as stress, anxiety, and lack of organizational support—factors that may affect the quality of care they provide [16]. Similarly, a study in Turkey reported that nurses caring for COVID-19 patients face problems such as burnout and social support deprivation [17]. COVID-19-related stressors negatively influence nurses’ psychological well-being, potentially compromising care quality. Consequently, this may affect the quality of nursing care.
The emergence of COVID-19 and the significant changes in healthcare delivery may have lasting effects on nurses’ perceptions, influencing them even after the pandemic has ended. Given that nurses have the most direct and prolonged contact with hospitalized COVID-19 patients, understanding their perception of care during this period may help improve patient outcomes. However, few studies have examined nurses’ multidimensional perceptions of COVID-19 care quality using validated scales like EPAECQC, during peak pandemic waves. Considering the uncertainty surrounding various aspects of the disease and nurses’ direct involvement in COVID-19 patient care, this study was designed to explore nurses’ perceptions of the quality of nursing care provided to patients with COVID-19.
Materials and Methods
Design and setting
This descriptive cross-sectional study included 204 participants. Participants were selected using a convenience sampling method. The research setting consisted of inpatient COVID-19 units in educational hospitals affiliated with Mazandaran University of Medical Sciences in the year 2020 (3 hospitals including Imam Khomeini Hospital, Razi Hospital and Boo'Ali Sina Hospital in Sari).
Inclusion and exclusion criteria
Inclusion criteria were: willingness to participate in the study, having at least an associate degree in nursing, and working in inpatient COVID-19 units and having more than six months of work experience. Exclusion criteria included incomplete questionnaire responses.
Data collection tools
Data were collected using a demographic questionnaire and The scale of perception of nursing activities that contribute to nursing care quality (EPAECQC). The demographic questionnaire included variables such as age, gender, marital status, education level, place of residence, income level, work experience, monthly working hours, shift type, and level of close contact with COVID-19 patients. The EPAECQC consists of 25 items covering 7 dimensions, measured on a 4-point Likert scale: Never (1), rarely (2), often (3), and always (4). The dimensions include: patient satisfaction (items 1–3), health promotion (items 4–6), prevention of complications (items 7–9), well-being and self-care (items 14 –16, and 18), functional readaptation (items 20–23), Nursing Care Organization (items 13 and 19), responsibility and rigor (items 10–12 and 17). The total score ranges from 25 to 100, with higher scores indicating higher perceived quality of nursing care. This questionnaire reflects the breadth of nursing activities and care quality. The reliability of the instrument was confirmed in a study by Ferreira Pereira da Silva Martins et al. with a Cronbach’s α coefficient of 0.94 [18]. In this study, we conducted face and content validity, which was confirmed. Two of the three validity stages were implemented. The reliability of this questionnaire was measured with a Cronbach’s α coefficient of 0.93. The validity and reliability of this questionnaire were also assessed in a study conducted in Tehran [19].
Data analysis
Data analysis was conducted using SPSS software version 26. Variables were described by percentage, mean, and standard deviation. In the nursing care quality questionnaire, the different dimensions consisted of varying numbers of items, leading to different potential total scores. To ensure comparability across all dimensions, the raw scores for each dimension were standardized and converted to a scale ranging from 0 to 100. Normality was assessed using skewness and kurtosis statistics. For all seven dimensions of nursing care quality, the absolute values of both skewness and kurtosis were below the threshold of 1; therefore, the assumption of normality was met for all variables. Comparison of mean nursing care quality scores across groups was performed using independent samples t-test and one-way ANOVA. Pearson correlation coefficients were calculated to assess the relationships between questionnaire dimensions. Finally, data were analyzed using Multivariate Regression Analysis. Model fit and goodness-of-fit were assessed through multiple diagnostic procedures, including examination of Q-Q plots for normality of standardized residuals, analysis of skewness and kurtosis statistics, variance inflation factors (all variance inflation factors (VIF) <5) to evaluate multicollinearity, and residual-versus-predicted value scatterplots to verify linearity assumptions. The significance level was set at 0.05.
Results
According to the findings, the mean age of participants was 35.15±6.94 years. Participant demographics including age, work experience, and monthly working hours are presented in Table 1. Table 1 also summarizes the comparison of nursing care quality scoresacross different demographic and occupational groups. Bivariate analyses revealed significant differences in outcome scores based on gender and work shift arrangements. As shown in Table 1, gender differences were significant (P=0.014). Similarly, healthcare workers with rotational shifts obtained significantly higher scores (78.1±11.9) than those with fixed shifts (72.3±14.6, P=0.024). No significant differences were found by marital status, education level, having children, employment status, place of residence, or income level (all P>0.05). However, a trend toward significance was noted for duration of contact with COVID-19 (P=0.094), with the more than 8 hours’ group showing the highest mean scores (83±9.7).
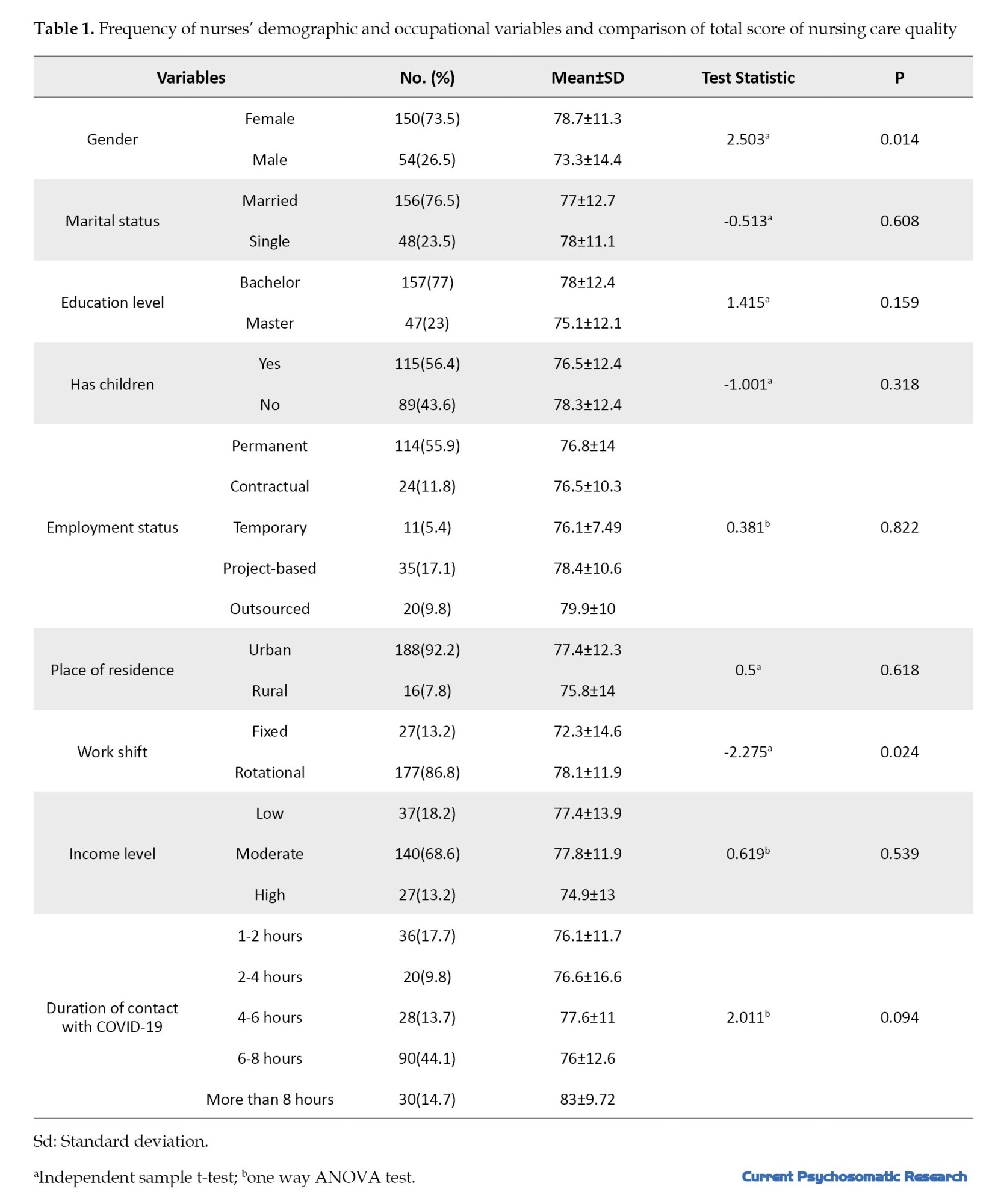
Figure 1 provides a graphical representation of the mean scores across the different dimensions of nursing care quality (to facilitate comparison, the scores were calculated on a 0 to 100 scale). The mean score for quality nursing care was 77.3±12.41. Among the dimensions of nursing care quality, responsibility and rigor had the highest mean score (79.6±13.3), followed by Nursing Care Organization (78.5±15.6), patient satisfaction (78.1±13.8) and well-being and self-care (77.3±16.2). Responsibility/rigor and organization scored highest, indicating sustained professional standards despite pandemic pressures.
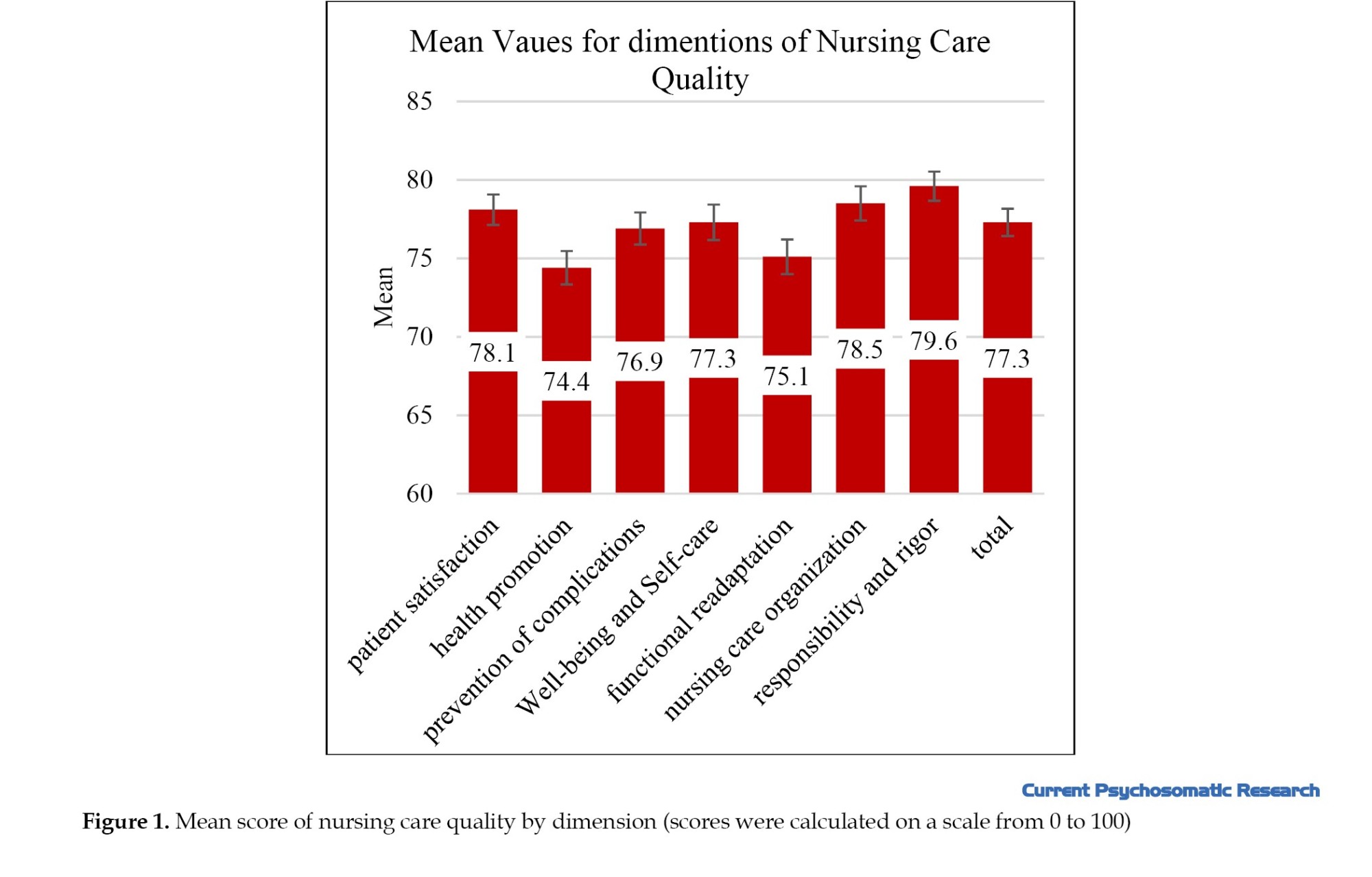
The dimension with the lowest score was health promotion (74.4±15.2), followed by functional readaptation (8.93±1.82) and prevention of complications (75.1±15.8).
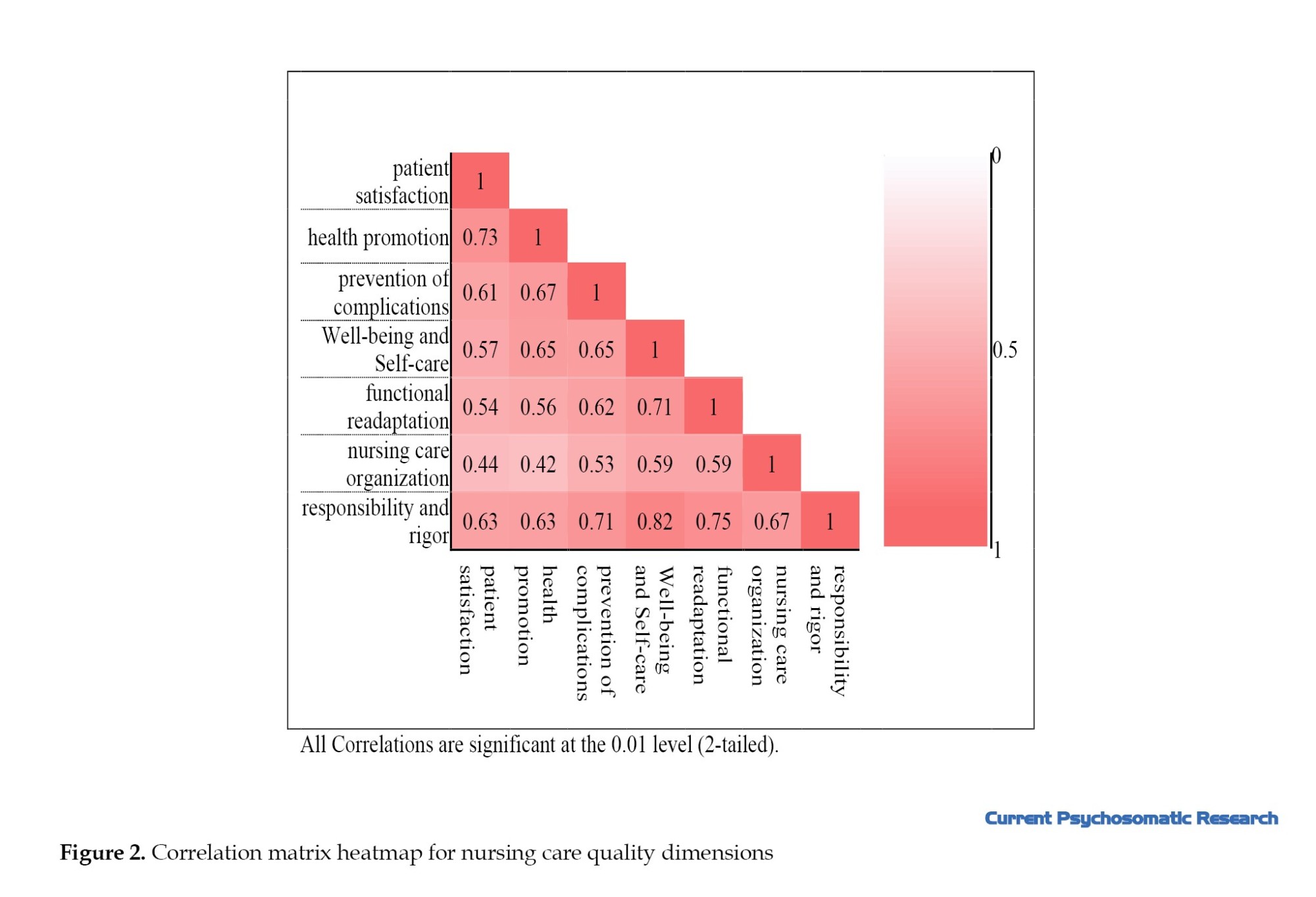
The heatmap in Figure 2 displays the correlation matrix among different dimensions of nursing care quality. Significant positive correlations were found between all pairs of dimensions, with correlation coefficients ranging from 0.418 to 0.815. The strongest correlations were observed between Responsibility and Rigor with Well-being and Self-care (r=0.815), and Prevention of Complications with Responsibility and Rigor (r=0.707). All correlations were statistically significant at P<0.001, indicating a strong interrelationship among the quality dimensions.
To examine the relationship between the study variables and dimensions of nursing care quality, multivariate regression analysis was employed. Initially, the association between each independent variable and the care quality dimensions was assessed individually. Variables with significant associations were then entered into a multiple model.
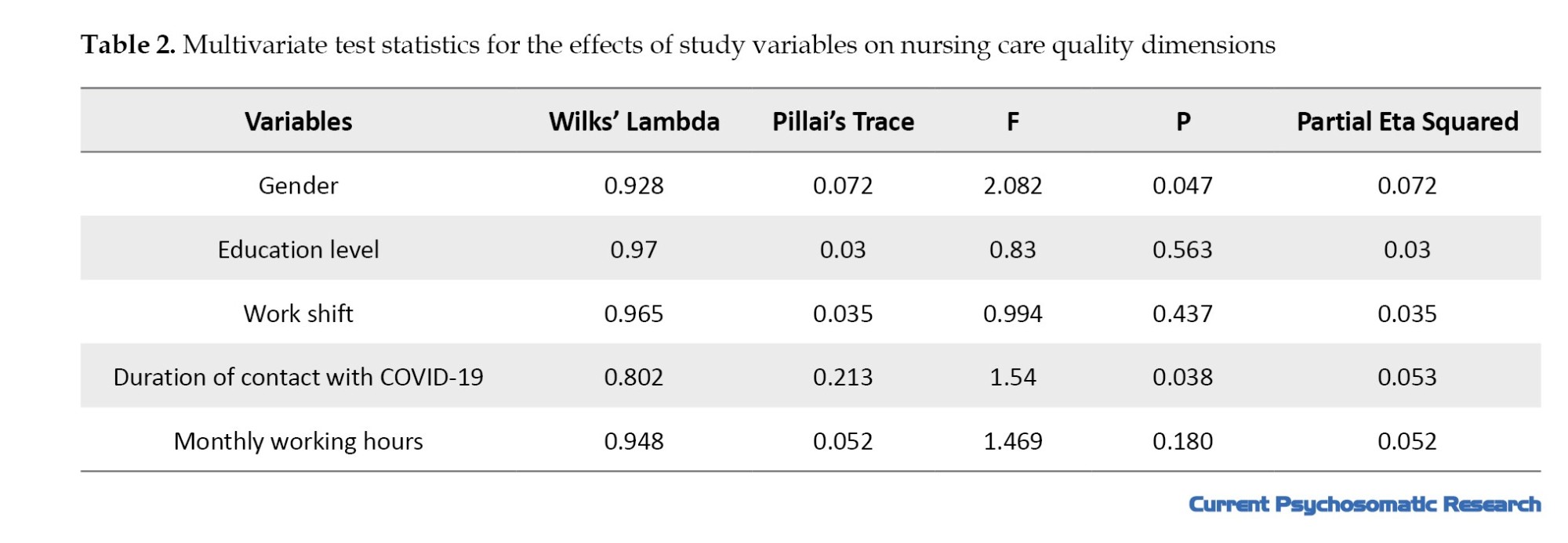
Multivariate analysis demonstrated that both sex and contact hours with COVID-19 patients had statistically significant effects on the combined scores of nursing care quality dimensions. Specifically, sex was associated with overall differences in care quality (Wilks’ Lambdas=0.928, Pillai’s traces=0.072, P=0.047), indicating that male and female nurses exhibited different performance profiles across the measured dimensions. Similarly, increased contact hours with COVID-19 patients were linked to significant differences in care quality (Wilks’ Lambdas=0.802, Pillai’s traces=0.213, P=0.038), suggesting that the level of exposure to COVID-19 was an important factor. Education level, work shift, and monthly working hours showed no significant multivariate associations with care quality dimensions (Table 2). The magnitude of the effects for sex and COVID-19 exposure was moderate, while other variables had small and nonsignificant impacts.
A more detailed multivariate analysis, controlling for other variables, is presented in Table 3, which shows the regression coefficients and significance levels for the relationships between each factor and the dimensions of the quality of nursing care. In the multivariate analysis, nurses’ gender showed a significant association with all dimensions of nursing care quality, even after controlling for other variables. In all dimensions, female nurses had higher quality of care scores compared to male nurses. Education level was significantly associated only with patient satisfaction, such that even after controlling for other variables, patient satisfaction among nurses with a bachelor’s degree was significantly higher than among those with a master’s degree. In examining the relationship between work shift and various dimensions of nursing care quality, after adjusting for other factors, work shift was significantly associated only with health promotion. Specifically, health promotion scores were significantly lower among nurses with fixed shifts compared to those with rotating shifts. Moreover, after controlling for other variables, monthly working hours were significantly associated with certain dimensions of nursing care quality. Accordingly, patient satisfaction, nursing care organization, and accountability and rigor were significantly higher among nurses with longer monthly working hours. Finally, after adjusting for other factors, the duration of exposure to COVID-19 was significantly related to some aspects of nursing care quality. Patient satisfaction among nurses who spent 6 to 8 hours per shift in COVID-19 wards was significantly lower than among those who spent more than 8 hours. Well-being and self-care were significantly lower among nurses who spent less than 6 hours per shift in COVID-19 units compared to those with more than 8 hours of exposure. Additionally, nursing care organization was significantly lower among nurses with 2 to 4 hours of contact with COVID-19 patients than those with over 8 hours. However, health promotion, prevention of complications, Functional readaptation, and accountability and rigor showed no significant association with the duration of contact with COVID-19 patients.
Comprehensive diagnostic analyses confirmed the adequacy of the multivariate regression model. Normality assumptions were met based on Q-Q plots and analyses of skewness and kurtosis of the standardized residuals across all dimensions. Multicollinearity was not problematic, as all VIF were below 5. Linearity between predictors and outcomes was supported by residuals versus predicted values plots. Adjusted R-squared values representing explained variance by the model were as follows: Patient satisfaction, 12.2%; health promotion, 7.0%; prevention of complications, 2.8%; well-being and self-care, 7.1%; functional readaptation, 2.4%; nursing care organization, 6.2%; and responsibility and rigor, 6.6%. These results indicate that the model provides a reasonable fit and moderate explanatory power for the variables studied.
Discussion
The aim of this study was to determine nurses’ perception of the quality of nursing care for patients with COVID-19. Consistent with Ebrahimi et al. and Gholjeh et al. studies [20, 21], participants demonstrated favorable perceptions despite pandemic pressures, suggesting Iranian nurses’ resilience and adaptation capacity during COVID-19 waves. Obregón-Gutiérrez et al., in a study on 225 nurses in Spain, also concluded that nurses’ perception of care quality was at a good level [22]. Another study on 394 nurses providing direct nursing care to patients during the COVID-19 pandemic indicated that 93.4% of the nurses reported very good/good quality of nursing care for overall in unit [7]. These findings could implicate high resilience among nurses caring for COVID-19 patients. Research has established a significant positive association between resilience and nurses’ work performance [23]. Resilience adaptively buffers the stress and anxiety stemming from the COVID-19 crisis [24].
Contrary to the findings of the present study, Lavoie-Tremblay et al. in Canada, in a study involving 1,705 nurses, found that nurses caring for COVID-19 patients reported higher chronic fatigue, lower job satisfaction, lower perceived care quality, and greater intention to leave their current position [25]. Which could be due to younger and educationally diverse sample of nurses (Table 1) in the present study compared to a lower percentage of graduate level nurses in the study mentioned previously. A study in 2019 reported that more educated nurses and better patient experiences of hospital care had a direct relationship. Nurses with a bachelor’s degree or higher education are generally better equipped to coordinate healthcare effectively. They tend to have stronger communication skills, sharper critical thinking abilities, and are more prepared to provide holistic, autonomous, evidence‐based care. This approach is essential for effectively addressing patients’ needs and ensuring the delivery of high-quality care [26].
According to the findings, in the multivariate analysis, nurses’ gender—after controlling for other variables—was significantly associated with all dimensions of nursing care quality. In all aspects, female nurses reported higher quality of care than their male counterparts. In contrast to the current findings, the study by katebi et al. on 63 nurses at Shohadah Qaen Hospital found no significant relationship between nurses’ and patients’ demographic characteristics (age, gender, clinical experience, residence, occupation, etc.) and quality of care scores [27]. However, the study by Khaki et al. (2018), which involved 210 nurses employed in educational hospitals affiliated with Shahid Beheshti University of Medical Sciences, also indicated a significant relationship between quality of nursing care and gender, in a way that the quality of nursing care was reported to be higher among female nurses compared to male nurses [28]. Professions evolve in social contexts shaped by stereotypes that influence perceptions and limit development. Nursing has long been tied to gender roles from its origins and broader societal divides. These views frame nurses through male-female distinctions and expectations of women’s caregiving roles. Such perceptions shape nurses’ self-concepts and career choices [29].
Our findings also revealed that education level was significantly associated only with patient satisfaction. Even after adjusting for other factors, patient satisfaction was significantly higher among nurses with bachelor’s degrees compared to those with master’s degrees. In contrast, Alrasheedi et al. In Saudi Arabia reported that nursing education level and years of experience were significant predictors of patient satisfaction and health outcomes in a government hospital. Nurses with higher education levels and more experience had higher patient satisfaction and better outcomes, including fewer safety incidents, infections, and falls [30]. This discrepancy might be due to the higher proportion of bachelor-level nurses (77%) in the current study, which may have influenced the results. Moreover, in Alrasheedi’s study, both years of experience and level of education were examined, whereas in the present study, years of work experience were not assessed.
This study has certain limitations, primarily its cross-sectional design, which constrains the extent to which causal inferences can be made, and the limited generalizability due to regional sampling bias. Data were collected from nurses working in specific healthcare settings, which may not represent broader populations. Another limitation was the reliance on self-reported questionnaires, which may be influenced by social desirability bias, particularly given the sensitive context of COVID-19 care. Additionally, data collection occurred during a specific wave of the COVID-19 pandemic, potentially affecting responses due to fluctuating workload and stress levels. Although nurses completed questionnaires while providing care under heavy workload, sufficient time was allocated to minimize response bias. Future longitudinal designs could address these constraints for more robust inferences
Conclusion
The findings of this study indicate a favorable level of nursing care quality for patients with COVID-19. Assessing nursing care quality among hospitalized patients offers critical insights for healthcare administrators to develop and implement targeted strategies that enhance patient satisfaction, improve working conditions for healthcare staff, and recognize the essential contributions of healthcare workers, particularly during crises like the COVID-19 pandemic. These results underscore the importance of ongoing quality monitoring and support for nursing staff to maintain high standards of care in challenging environments. Future research should explore longitudinal changes in care quality perceptions and investigate interventions that effectively sustain and improve nursing care during and beyond pandemic conditions.
Ethical Considerations
Compliance with ethical guidelines
Before obtaining informed consent, the overall aims of the study were explained to participants, and they were assured of the confidentiality of their information. This study was approved by the Ethics Committee of the Vice Chancellor for Research and Technology at Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1399.597).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and study design, data collection and analysis, interpretation of the results, and manuscript drafting. All authors approved the submission of the final version of the manuscript.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We express our sincere gratitude to all the officials at Mazandaran University of Medical Sciences and the nurses who supported us throughout this research.
References
Ensuring and enhancing the quality of nursing care stands as a critical and ongoing challenge for healthcare systems globally, demanding continuous commitment and innovation to meet the evolving needs of patients [1]. The nurses’ professional expertise and experience are critical predictors of high-quality care [2]. Nurses are the primary agents of care quality; therefore, their perception of care quality should be taken seriously. Emerging studies have shown that both job satisfaction and nurses’ intention to leave the profession influence their perceptions of care quality [3]. Nurses may consider leaving their positions to seek more favorable environments when they perceive that their current working conditions fail to support professional standards [4]. Nurses’ insights into care quality and improvement strategies evolve through ongoing bedside practice. These perceptions reliably indicate actual care delivered. Assessing care quality via nurses’ views thereby evaluates treatment success and patient care standards [5].
During times of crisis, it is essential to understand how changes in providing healthcare impact healthcare professionals. As COVID-19, the acute respiratory syndrome, has fluctuated across countries, medical resources have remained uncertain, and healthcare priorities, policies and procedures have rapidly changed [6]. Because of the pandemic, nurses in hospital environments frequently worked extended hours and managed exceptionally high patient volumes, with limited chances for rest or recuperation [7]. In addition to facing these challenges, healthcare providers often struggle to balance their responsibilities toward patients, their families, and themselves. This dynamic, stressful, and uncertain environment can lead to situations where ethical values or obligations are compromised [6]. Healthcare workers may face situations where external factors like resource constraints, new health policies, or care models prevent them from acting in line with their core ethical beliefs. They often recognize ethical conflicts but feel powerless to maintain ethical standards due to these pressures. This results in a compromise of their professional integrity [8]. When such circumstances are repeated frequently, they can result in “moral injury”, exacerbating emotional distress, burnout, and frustration, and ultimately leading to workforce attrition [9].
Since the onset of COVID-19 in 2019, a major transformation has occurred in providing healthcare for professionals working in this field, significantly altering routine care practices [10, 11]. The intense workload in high-risk environments has even affected nursing care for non-COVID-19 patients [12, 13]. Healthcare workers have played a vital role in facilitating these changes and reported a wide range of experiences [14, 15]. Investigations into the care of patients with COVID-19 have highlighted the challenges in this area. Research conducted in Iran has shown that nurses caring for COVID-19 patients experience issues such as stress, anxiety, and lack of organizational support—factors that may affect the quality of care they provide [16]. Similarly, a study in Turkey reported that nurses caring for COVID-19 patients face problems such as burnout and social support deprivation [17]. COVID-19-related stressors negatively influence nurses’ psychological well-being, potentially compromising care quality. Consequently, this may affect the quality of nursing care.
The emergence of COVID-19 and the significant changes in healthcare delivery may have lasting effects on nurses’ perceptions, influencing them even after the pandemic has ended. Given that nurses have the most direct and prolonged contact with hospitalized COVID-19 patients, understanding their perception of care during this period may help improve patient outcomes. However, few studies have examined nurses’ multidimensional perceptions of COVID-19 care quality using validated scales like EPAECQC, during peak pandemic waves. Considering the uncertainty surrounding various aspects of the disease and nurses’ direct involvement in COVID-19 patient care, this study was designed to explore nurses’ perceptions of the quality of nursing care provided to patients with COVID-19.
Materials and Methods
Design and setting
This descriptive cross-sectional study included 204 participants. Participants were selected using a convenience sampling method. The research setting consisted of inpatient COVID-19 units in educational hospitals affiliated with Mazandaran University of Medical Sciences in the year 2020 (3 hospitals including Imam Khomeini Hospital, Razi Hospital and Boo'Ali Sina Hospital in Sari).
Inclusion and exclusion criteria
Inclusion criteria were: willingness to participate in the study, having at least an associate degree in nursing, and working in inpatient COVID-19 units and having more than six months of work experience. Exclusion criteria included incomplete questionnaire responses.
Data collection tools
Data were collected using a demographic questionnaire and The scale of perception of nursing activities that contribute to nursing care quality (EPAECQC). The demographic questionnaire included variables such as age, gender, marital status, education level, place of residence, income level, work experience, monthly working hours, shift type, and level of close contact with COVID-19 patients. The EPAECQC consists of 25 items covering 7 dimensions, measured on a 4-point Likert scale: Never (1), rarely (2), often (3), and always (4). The dimensions include: patient satisfaction (items 1–3), health promotion (items 4–6), prevention of complications (items 7–9), well-being and self-care (items 14 –16, and 18), functional readaptation (items 20–23), Nursing Care Organization (items 13 and 19), responsibility and rigor (items 10–12 and 17). The total score ranges from 25 to 100, with higher scores indicating higher perceived quality of nursing care. This questionnaire reflects the breadth of nursing activities and care quality. The reliability of the instrument was confirmed in a study by Ferreira Pereira da Silva Martins et al. with a Cronbach’s α coefficient of 0.94 [18]. In this study, we conducted face and content validity, which was confirmed. Two of the three validity stages were implemented. The reliability of this questionnaire was measured with a Cronbach’s α coefficient of 0.93. The validity and reliability of this questionnaire were also assessed in a study conducted in Tehran [19].
Data analysis
Data analysis was conducted using SPSS software version 26. Variables were described by percentage, mean, and standard deviation. In the nursing care quality questionnaire, the different dimensions consisted of varying numbers of items, leading to different potential total scores. To ensure comparability across all dimensions, the raw scores for each dimension were standardized and converted to a scale ranging from 0 to 100. Normality was assessed using skewness and kurtosis statistics. For all seven dimensions of nursing care quality, the absolute values of both skewness and kurtosis were below the threshold of 1; therefore, the assumption of normality was met for all variables. Comparison of mean nursing care quality scores across groups was performed using independent samples t-test and one-way ANOVA. Pearson correlation coefficients were calculated to assess the relationships between questionnaire dimensions. Finally, data were analyzed using Multivariate Regression Analysis. Model fit and goodness-of-fit were assessed through multiple diagnostic procedures, including examination of Q-Q plots for normality of standardized residuals, analysis of skewness and kurtosis statistics, variance inflation factors (all variance inflation factors (VIF) <5) to evaluate multicollinearity, and residual-versus-predicted value scatterplots to verify linearity assumptions. The significance level was set at 0.05.
Results
According to the findings, the mean age of participants was 35.15±6.94 years. Participant demographics including age, work experience, and monthly working hours are presented in Table 1. Table 1 also summarizes the comparison of nursing care quality scoresacross different demographic and occupational groups. Bivariate analyses revealed significant differences in outcome scores based on gender and work shift arrangements. As shown in Table 1, gender differences were significant (P=0.014). Similarly, healthcare workers with rotational shifts obtained significantly higher scores (78.1±11.9) than those with fixed shifts (72.3±14.6, P=0.024). No significant differences were found by marital status, education level, having children, employment status, place of residence, or income level (all P>0.05). However, a trend toward significance was noted for duration of contact with COVID-19 (P=0.094), with the more than 8 hours’ group showing the highest mean scores (83±9.7).
Figure 1 provides a graphical representation of the mean scores across the different dimensions of nursing care quality (to facilitate comparison, the scores were calculated on a 0 to 100 scale). The mean score for quality nursing care was 77.3±12.41. Among the dimensions of nursing care quality, responsibility and rigor had the highest mean score (79.6±13.3), followed by Nursing Care Organization (78.5±15.6), patient satisfaction (78.1±13.8) and well-being and self-care (77.3±16.2). Responsibility/rigor and organization scored highest, indicating sustained professional standards despite pandemic pressures.
The dimension with the lowest score was health promotion (74.4±15.2), followed by functional readaptation (8.93±1.82) and prevention of complications (75.1±15.8).
The heatmap in Figure 2 displays the correlation matrix among different dimensions of nursing care quality. Significant positive correlations were found between all pairs of dimensions, with correlation coefficients ranging from 0.418 to 0.815. The strongest correlations were observed between Responsibility and Rigor with Well-being and Self-care (r=0.815), and Prevention of Complications with Responsibility and Rigor (r=0.707). All correlations were statistically significant at P<0.001, indicating a strong interrelationship among the quality dimensions.
To examine the relationship between the study variables and dimensions of nursing care quality, multivariate regression analysis was employed. Initially, the association between each independent variable and the care quality dimensions was assessed individually. Variables with significant associations were then entered into a multiple model.
Multivariate analysis demonstrated that both sex and contact hours with COVID-19 patients had statistically significant effects on the combined scores of nursing care quality dimensions. Specifically, sex was associated with overall differences in care quality (Wilks’ Lambdas=0.928, Pillai’s traces=0.072, P=0.047), indicating that male and female nurses exhibited different performance profiles across the measured dimensions. Similarly, increased contact hours with COVID-19 patients were linked to significant differences in care quality (Wilks’ Lambdas=0.802, Pillai’s traces=0.213, P=0.038), suggesting that the level of exposure to COVID-19 was an important factor. Education level, work shift, and monthly working hours showed no significant multivariate associations with care quality dimensions (Table 2). The magnitude of the effects for sex and COVID-19 exposure was moderate, while other variables had small and nonsignificant impacts.
A more detailed multivariate analysis, controlling for other variables, is presented in Table 3, which shows the regression coefficients and significance levels for the relationships between each factor and the dimensions of the quality of nursing care. In the multivariate analysis, nurses’ gender showed a significant association with all dimensions of nursing care quality, even after controlling for other variables. In all dimensions, female nurses had higher quality of care scores compared to male nurses. Education level was significantly associated only with patient satisfaction, such that even after controlling for other variables, patient satisfaction among nurses with a bachelor’s degree was significantly higher than among those with a master’s degree. In examining the relationship between work shift and various dimensions of nursing care quality, after adjusting for other factors, work shift was significantly associated only with health promotion. Specifically, health promotion scores were significantly lower among nurses with fixed shifts compared to those with rotating shifts. Moreover, after controlling for other variables, monthly working hours were significantly associated with certain dimensions of nursing care quality. Accordingly, patient satisfaction, nursing care organization, and accountability and rigor were significantly higher among nurses with longer monthly working hours. Finally, after adjusting for other factors, the duration of exposure to COVID-19 was significantly related to some aspects of nursing care quality. Patient satisfaction among nurses who spent 6 to 8 hours per shift in COVID-19 wards was significantly lower than among those who spent more than 8 hours. Well-being and self-care were significantly lower among nurses who spent less than 6 hours per shift in COVID-19 units compared to those with more than 8 hours of exposure. Additionally, nursing care organization was significantly lower among nurses with 2 to 4 hours of contact with COVID-19 patients than those with over 8 hours. However, health promotion, prevention of complications, Functional readaptation, and accountability and rigor showed no significant association with the duration of contact with COVID-19 patients.
Comprehensive diagnostic analyses confirmed the adequacy of the multivariate regression model. Normality assumptions were met based on Q-Q plots and analyses of skewness and kurtosis of the standardized residuals across all dimensions. Multicollinearity was not problematic, as all VIF were below 5. Linearity between predictors and outcomes was supported by residuals versus predicted values plots. Adjusted R-squared values representing explained variance by the model were as follows: Patient satisfaction, 12.2%; health promotion, 7.0%; prevention of complications, 2.8%; well-being and self-care, 7.1%; functional readaptation, 2.4%; nursing care organization, 6.2%; and responsibility and rigor, 6.6%. These results indicate that the model provides a reasonable fit and moderate explanatory power for the variables studied.
Discussion
The aim of this study was to determine nurses’ perception of the quality of nursing care for patients with COVID-19. Consistent with Ebrahimi et al. and Gholjeh et al. studies [20, 21], participants demonstrated favorable perceptions despite pandemic pressures, suggesting Iranian nurses’ resilience and adaptation capacity during COVID-19 waves. Obregón-Gutiérrez et al., in a study on 225 nurses in Spain, also concluded that nurses’ perception of care quality was at a good level [22]. Another study on 394 nurses providing direct nursing care to patients during the COVID-19 pandemic indicated that 93.4% of the nurses reported very good/good quality of nursing care for overall in unit [7]. These findings could implicate high resilience among nurses caring for COVID-19 patients. Research has established a significant positive association between resilience and nurses’ work performance [23]. Resilience adaptively buffers the stress and anxiety stemming from the COVID-19 crisis [24].
Contrary to the findings of the present study, Lavoie-Tremblay et al. in Canada, in a study involving 1,705 nurses, found that nurses caring for COVID-19 patients reported higher chronic fatigue, lower job satisfaction, lower perceived care quality, and greater intention to leave their current position [25]. Which could be due to younger and educationally diverse sample of nurses (Table 1) in the present study compared to a lower percentage of graduate level nurses in the study mentioned previously. A study in 2019 reported that more educated nurses and better patient experiences of hospital care had a direct relationship. Nurses with a bachelor’s degree or higher education are generally better equipped to coordinate healthcare effectively. They tend to have stronger communication skills, sharper critical thinking abilities, and are more prepared to provide holistic, autonomous, evidence‐based care. This approach is essential for effectively addressing patients’ needs and ensuring the delivery of high-quality care [26].
According to the findings, in the multivariate analysis, nurses’ gender—after controlling for other variables—was significantly associated with all dimensions of nursing care quality. In all aspects, female nurses reported higher quality of care than their male counterparts. In contrast to the current findings, the study by katebi et al. on 63 nurses at Shohadah Qaen Hospital found no significant relationship between nurses’ and patients’ demographic characteristics (age, gender, clinical experience, residence, occupation, etc.) and quality of care scores [27]. However, the study by Khaki et al. (2018), which involved 210 nurses employed in educational hospitals affiliated with Shahid Beheshti University of Medical Sciences, also indicated a significant relationship between quality of nursing care and gender, in a way that the quality of nursing care was reported to be higher among female nurses compared to male nurses [28]. Professions evolve in social contexts shaped by stereotypes that influence perceptions and limit development. Nursing has long been tied to gender roles from its origins and broader societal divides. These views frame nurses through male-female distinctions and expectations of women’s caregiving roles. Such perceptions shape nurses’ self-concepts and career choices [29].
Our findings also revealed that education level was significantly associated only with patient satisfaction. Even after adjusting for other factors, patient satisfaction was significantly higher among nurses with bachelor’s degrees compared to those with master’s degrees. In contrast, Alrasheedi et al. In Saudi Arabia reported that nursing education level and years of experience were significant predictors of patient satisfaction and health outcomes in a government hospital. Nurses with higher education levels and more experience had higher patient satisfaction and better outcomes, including fewer safety incidents, infections, and falls [30]. This discrepancy might be due to the higher proportion of bachelor-level nurses (77%) in the current study, which may have influenced the results. Moreover, in Alrasheedi’s study, both years of experience and level of education were examined, whereas in the present study, years of work experience were not assessed.
This study has certain limitations, primarily its cross-sectional design, which constrains the extent to which causal inferences can be made, and the limited generalizability due to regional sampling bias. Data were collected from nurses working in specific healthcare settings, which may not represent broader populations. Another limitation was the reliance on self-reported questionnaires, which may be influenced by social desirability bias, particularly given the sensitive context of COVID-19 care. Additionally, data collection occurred during a specific wave of the COVID-19 pandemic, potentially affecting responses due to fluctuating workload and stress levels. Although nurses completed questionnaires while providing care under heavy workload, sufficient time was allocated to minimize response bias. Future longitudinal designs could address these constraints for more robust inferences
Conclusion
The findings of this study indicate a favorable level of nursing care quality for patients with COVID-19. Assessing nursing care quality among hospitalized patients offers critical insights for healthcare administrators to develop and implement targeted strategies that enhance patient satisfaction, improve working conditions for healthcare staff, and recognize the essential contributions of healthcare workers, particularly during crises like the COVID-19 pandemic. These results underscore the importance of ongoing quality monitoring and support for nursing staff to maintain high standards of care in challenging environments. Future research should explore longitudinal changes in care quality perceptions and investigate interventions that effectively sustain and improve nursing care during and beyond pandemic conditions.
Ethical Considerations
Compliance with ethical guidelines
Before obtaining informed consent, the overall aims of the study were explained to participants, and they were assured of the confidentiality of their information. This study was approved by the Ethics Committee of the Vice Chancellor for Research and Technology at Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1399.597).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and study design, data collection and analysis, interpretation of the results, and manuscript drafting. All authors approved the submission of the final version of the manuscript.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We express our sincere gratitude to all the officials at Mazandaran University of Medical Sciences and the nurses who supported us throughout this research.
References
- Maghsoud F, Rezaei M, Asgarian FS, Rassouli M. Workload and quality of nursing care: The mediating role of implicit rationing of nursing care, job satisfaction and emotional exhaustion by using structural equations modeling approach. BMC Nurs. 2022; 21(1):273. [DOI:10.1186/s12912-022-01055-1] [PMID]
- Spence Laschinger HK, Zhu J, Read E. New nurses’ perceptions of professional practice behaviours, quality of care, job satisfaction and career retention. J Nurs Manag. 2016; 24(5):656-65. [DOI:10.1111/jonm.12370] [PMID]
- Laschinger HKS, Fida R. Linking nurses’ perceptions of patient care quality to job satisfaction: The role of authentic leadership and empowering professional practice environments. J Nurs Adm. 2015; 45(5):276-83. [DOI:10.1097/NNA.0000000000000198] [PMID]
- Cao T, Huang X, Wang L, Li B, Dong X, Lu H, et al. Effects of organisational justice, work engagement and nurses’ perception of care quality on turnover intention among newly licensed registered nurses: A structural equation modelling approach. J Clin Nurs. 2020; 29(13-14):2626-37. [DOI:10.1111/jocn.15285] [PMID]
- Alilyyani B, Kerr M, Wong C, Wazqar D. A psychometric analysis of the nurse satisfaction with the quality of care scale. Healthcare. 2022; 10(6):1145. [DOI:10.3390/healthcare10061145] [PMID]
- Rushton CH, Doerries B, Greene J, Geller G. Dramatic interventions in the tragedy of the COVID-19 pandemic. Lancet. 2020; 396(10247):305-6. [DOI:10.1016/S0140-6736(20)31641-X] [PMID]
- Nantsupawat A, Wichaikhum OA, Abhicharttibutra K, Sadarangani T, Poghosyan L. The relationship between nurse burnout, missed nursing care, and care quality following COVID‐19 pandemic. J Clin Nurs. 2023; 32(15-16):5076-83. [DOI:10.1111/jocn.16761] [PMID]
- Rushton CH. Moral resilience: A capacity for navigating moral distress in critical care. AACN Adv Crit Care. 2016; 27(1):111-9. [DOI:10.4037/aacnacc2016275] [PMID]
- Ducharlet K, Philip J, Gock H, Brown M, Gelfand SL, Josland EA, et al. Moral distress in nephrology: Perceived barriers to ethical clinical care. Am J Kidney Dis. 2020; 76(2):248-54. [DOI:10.1053/j.ajkd.2019.09.018] [PMID]
- Ripp J, Peccoralo L, Charney D. Attending to the emotional well-being of the health care workforce in a New York City health system during the COVID-19 pandemic. Acad Med. 2020. [DOI:10.1097/ACM.0000000000003414] [PMID]
- Huang J, Liu F, Teng Z, Chen J, Zhao J, Wang X, et al. Care for the psychological status of frontline medical staff fighting against Coronavirus Disease 2019 (COVID-19). Clin Infect Dis. 2020; 71(12):3268-9. [DOI:10.1093/cid/ciaa385] [PMID]
- Marten R, Mikkelsen B, Shao R, Dal Zennaro L, Berdzuli N, Fernando T, et al. Committing to implementation research for health systems to manage and control non-communicable diseases. Lancet Glob Health. 2021; 9(2):e108-e9. [DOI:10.1016/S2214-109X(20)30485-X] [PMID]
- Chudasama YV, Gillies CL, Zaccardi F, Coles B, Davies MJ, Seidu S, et al. Impact of COVID-19 on routine care for chronic diseases: A global survey of views from healthcare professionals. Diabetes Metab Syndr. 2020; 14(5):965-7. [DOI:10.1016/j.dsx.2020.06.042] [PMID]
- Webster P. Virtual health care in the era of COVID-19. Lancet. 2020; 395(10231):1180-1. [DOI:10.1016/S0140-6736(20)30818-7] [PMID]
- Hartzband P, Groopman J. Physician burnout, interrupted. N Engl J Med. 2020; 382(26):2485-7. [DOI:10.1056/NEJMp2003149] [PMID]
- Karimi Z, Fereidouni Z, Behnammoghadam M, Alimohammadi N, Mousavizadeh A, Salehi T, et al. The lived experience of nurses caring for patients with COVID-19 in Iran: A phenomenological study. Risk Manag Healthc Policy. 2020; 13:1271. [DOI:10.2147/RMHP.S258785] [PMID]
- Kackin O, Ciydem E, Aci OS, Kutlu FY. Experiences and psychosocial problems of nurses caring for patients diagnosed with COVID-19 in Turkey: A qualitative study. Int J Soc Psychiatry. 2021; 67(2):158-67. [DOI:10.1177/0020764020942788] [PMID]
- Ferreira Pereira da Silva Martins MM, da Costa Gonçalves MN, Pimenta Lopes Ribeiro OM, Rizatto Tronchin DM. Quality of nursing care: Instrument development and validation. Rev Bras Enferm. 2016; 69(5). [DOI:10.1590/0034-7167-2015-0151] [PMID]
- Khachian A, Rezaei M, Haroonzadeh R, Haghani S, Salehi T. The perception of nurses about the quality of nursing services in nurses working in medical education centers of Iran University of Medical Sciences. Iran J Nurs. 2024; 37(150):380-91. [DOI:10.32598/ijn.37.150.3008]
- Ebrahimi F, Jafarjalal E, Najafi Ghezeljeh T, Haghani S. The quality of nursing care in nurses working in the intensive care unit of COVID-19 in Arak medical training centers in 2021-2022. Hayat. 2023; 29(1):89-100.
- Gholjeh M, Dastoorpour M, Ghasemi A. The relationship between nursing care quality and patients satisfaction among hospitals affiliated to Zahedan University of Medical Sciences in 2014. Jorjani Biomed J. 2015; 3(1):68-81.
- Obregón-Gutiérrez N, Puig-Calsina S, Bonfill-Abella A, Forrellat-González L, Subirana-Casacuberta M. “Care left undone” and quality of care during the COVID-19 pandemic: Influential factors and modulating strategies. Enferm Clin. 2022; 32(1):4-11. [DOI:10.1016/j.enfcle.2021.06.004] [PMID]
- Walpita YN, Arambepola C. High resilience leads to better work performance in nurses: Evidence from South Asia. J Nurs Manag. 2020; 28(2):342-50. [DOI:10.1111/jonm.12930] [PMID]
- Aghamohammadi F, Saed O, Dinmohammadi M. Factors affecting the resilience of Iranian nurses during the COVID-19 Pandemic. J Client-Centered Nurs Care. 2023; 9(3):223-30. [DOI:10.32598/JCCNC.9.3.451]
- Lavoie‐Tremblay M, Gélinas C, Aubé T, Tchouaket E, Tremblay D, Gagnon MP, et al. Influence of caring for COVID‐19 patients on nurse’s turnover, work satisfaction and quality of care. J Nurs Manag. 2022; 30(1):33-43. [DOI:10.1111/jonm.13462] [PMID]
- Liu X, Zheng J, Liu K, Baggs JG, Liu J, Wu Y, et al. Associations of nurse education level and nurse staffing with patient experiences of hospital care: A cross sectional study in China. Res Nurs Health. 2020; 43(1):103-13. [DOI:10.1002/nur.22003] [PMID]
- Katebi MS, Ghalenoei M, Zalbeiki S, Barzegari Esfeden Z. Quality of patient care from the viewpoint of nurses and patients in the teaching hospitals of Shohadah Qaen. J Sabzevar Univ Med Sci. 2021; 28(3):339-46.
- Khaki S, Esmaeilpourzanjani S, Mashouf S. Nursing cares quality in nurses. SJNMP. 2018; 3(4):1-14. [DOI:10.29252/sjnmp.3.4.1]
- Teresa-Morales C, Rodríguez-Pérez M, Araujo-Hernández M, Feria-Ramírez C. Current stereotypes associated with nursing and nursing professionals: An integrative review. Int J Environ Res Public Health. 2022; 19(13):7640. [DOI:10.3390/ijerph19137640] [PMID]
- Alrasheedi FN, Al Rasheedi MS, Alrasheedy SKD, Alrasheed AKD, Al Rashedi TNA, Al Rasheedi AS. The relationship between nursing education level and years of experience on patient satisfaction and health outcomes in a public hospital in Saudi Arabia. Chelonian Research Foundation. Chelonian Res Found. 2022; 17(2):3549-57. [Doi:10.18011/2022.04(1) 3549-3557]
Type of Study: Research |
Subject:
Health services management
Received: 2024/06/10 | Accepted: 2024/08/13 | Published: 2024/10/1
Received: 2024/06/10 | Accepted: 2024/08/13 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
