Wed, May 27, 2026
[Archive]
Volume 3, Issue 1 (Autumn 2024)
CPR 2024, 3(1): 33-40 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gholipour N, Ghanbari A, Esmaeili R, Nazari R, Sharif-Nia H. Nurses’ Resilience and Intention to Care for COVID-19 Patients: The Role of Demographic Factors. CPR 2024; 3 (1) :33-40
URL: http://cpr.mazums.ac.ir/article-1-130-en.html
URL: http://cpr.mazums.ac.ir/article-1-130-en.html



Orthopedic Research Center, Mazandaran University of Medical Sciences, Sari, Iran.
Full-Text [PDF 612 kb]
(32 Downloads)
| Abstract (HTML) (99 Views)
Full-Text: (19 Views)
Introduction
The COVID-19 pandemic first began in Wuhan, China, in December 2019, and the deadly virus rapidly spread across the globe, quickly becoming a global health crisis [1, 2]. According to the latest report from the World Health Organization (WHO), by the end of July 2024, more than 775 million people worldwide had been infected with the virus, and, unfortunately, over 7 million had died. During the same period, Iran was also affected by this crisis, reporting more than 7.5 million cases and about 147,000 deaths [3]. These alarming statistics highlight the extent and severity of this global crisis.
The widespread infection of COVID-19 within communities poses a unique professional challenge for the healthcare systems of each country. In particular, members of the healthcare team, especially nurses, are on the front lines of the fight against this disease and require significant attention and support [4]. During this crisis, the workload in many hospital departments has increased dramatically, and nurses have been faced with a high volume of patients on a daily basis [5].
The decrease in nurses’ intention to care for COVID-19 patients, especially in crisis situations, could be considered one of the factors affecting the quality of care and the efficiency of the healthcare system. Consequently, identifying the factors that may influence nurses’ intention is an important step toward planning and managing human resources in similar future crises [6].
A nurse’s intention to provide care during a pandemic can be influenced by various individual and organizational factors [7]. Among individual factors, demographic characteristics such as age, gender, marital status, work history, vaccination status, COVID-19 history, and education level have been identified as important variables in predicting nurses’ behavior and their intention to care for patients. For example, Yang et al. and Joseph identified factors such as age and work experience as significant predictors of nurses’ intention to continue working, with more experienced employees demonstrating a greater intention to remain in their roles [8, 9]. Additionally, the study by Kohestani et al. and Al-Hunaishi et al. showed that gender and higher education levels had a significant impact on nurses’ intention to care for COVID-19 patients [10, 11]. These findings highlight the complex interplay of demographic factors influencing nurses’ intention to work in high-risk environments; however, results in this area are not always consistent and can vary based on geographical and cultural contexts.
In addition to demographic characteristics, resilience has also been recognized as an important human ability in coping with occupational stress and health crises. Resilience, defined as the ability to be flexible and return to psychological balance after facing difficult situations, has been identified in numerous studies as a factor that enhances the mental health and professional performance of nurses in critical situations [12]. During the COVID-19 pandemic, resilience has emerged as a key component in maintaining the mental health of nurses. Various studies in different countries have shown that nurses, despite experiencing severe psychological stress, often report moderate to high levels of resilience. For example, a study conducted in Thailand found that high resilience was associated with a reduced tendency to leave the nursing profession [13]. Additionally, research results from Iran indicate that the level of resilience among nurses during different waves of the pandemic was moderate [14, 15].
Recognizing the importance of assessing nurses’ intention to care for patients during the COVID-19 pandemic, as well as the influential role of psychological characteristics like resilience, this study aimed to investigate the relationship between nurses’ resilience and their intention to care for COVID-19 patients. The impact of certain demographic characteristics on this relationship was also analyzed. The results can assist policymakers and health managers in designing and implementing effective programs to support nurses and enhance the quality of health care in critical situations.
Materials and Methods
This descriptive-analytical correlational study was conducted on nurses caring for COVID-19 patients in public hospitals in Amol in 2021. G*Power software, version 3.1 was utilized to ensure an adequate sample size. Considering an effect size of 0.06, a significance level of 0.05, and a test power of 80%, the required sample size was determined to be 215 individuals. The inclusion criteria specified a minimum of 12 months of nursing work experience. This criterion was established to ensure that nurses had sufficient experience in the hospital setting and were familiar with the specific challenges of caring for COVID-19 patients, as indicated by the study conducted by Afshari et al. [14]. This approach will help collect more accurate data and better assess nurses’ intention to care for these patients.
Data were collected using a three-part form. The first part included a demographic checklist that gathered information such as age, gender, marital status, education level, work experience, type of employment, vaccination history, and COVID-19 infection. The second part comprised the Connor–Davidson resilience scale (CD-RISC) [16]. This questionnaire consists of 25 items divided into 5 subscales: Personal competence and efficacy (8 items), tolerance of negative effects and resilience to stress (7 items), positive acceptance of change (5 items), self-control (3 items), and spiritual influences (2 items). The items are scored on a five-point Likert scale as follows: (Completely false=0), (rarely=1), (sometimes true=2), (often true=3), and (always true=4). The highest score an individual can achieve is 100, while the lowest score is zero. A high score on this test indicates a high level of resilience. In this study, the reliability of the instrument was estimated to be 0.914 using Cronbach’s α. The third section included the Nurses’ Intention to Care Scale (NICS), designed by Yoo et al. in 2005 [17]. Responses are scored on a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). This tool is structured into three dimensions: Behavioral beliefs (14 items), social norms (8 items), and belief control (18 items). Test scores range from 40 to 280, with higher scores indicating a greater tendency for nurses to provide higher levels of care. This tool has been psychometrically validated in Persian by Rahmatpour et al. who demonstrated that the factor structure of this instrument accounts for 53.12% of the variance in the concept of intention to care for COVID patients in the Iranian context. Additionally, the values of Cronbach’s α, McDonald’s omega, CR, and maximum reliability of the extracted factors have been reported to exceed 0.8 [18]. In this study, the reliability of the instrument was estimated to be 0.929 using Cronbach’s α.
Procedure
After the research was approved by the Research Council of Mazandaran University of Medical Sciences and received approval from the Ethics Committee, the questionnaires were initially prepared online by uploading them to the Pressline website, and the relevant link was shared in the WhatsApp group for nurses in the target community. However, due to the relatively low participation rate in the online format, the principal investigator, with an official letter of introduction from the university, visited all four hospitals in Amol City—Imam Reza (AS), 17 Shahrivar, Imam Khomeini (RA), and Imam Ali (AS)—which were treating COVID-19 patients at that time. In the in-person format, the researcher physically distributed the questionnaires to volunteer nurses after explaining the study’s objectives. To maintain ethical standards and prevent bias, the questionnaires were completed in a self-administered manner in a separate environment, with the researcher present only for initial guidance and the distribution of the forms. In total, approximately 28% of the sample completed the questionnaires online, while 72% did so in person. Relative quota allocation in the distribution of questionnaires was based on the number of active nurses in the COVID-19 inpatient wards of each hospital.
Data analysis
Data were analyzed using SPSS software, version 26. The normality of data distribution was examined using the Kolmogorov-Smirnov test, which indicated that all main variables followed a normal distribution. Descriptive statistics (Mean±SD, frequency, and percentage) were employed to summarize the data. In the inferential statistics section, an independent t-test and ANOVA were utilized to compare the mean scores of resilience and caregiving tendency between two and multiple groups, respectively. The Pearson correlation test was conducted to examine the relationship between resilience scores and caregiving tendency, while simple linear regression was applied to analyze the predictor variables of intention to care. Additionally, the assumptions of the regression test, including data normality, absence of multicollinearity, and homogeneity of variances, were assessed, and all these assumptions were met. Furthermore, a confidence coefficient of 95% (α=5%), a significance level of 0.05, and a test power of 80% (β=20%) were considered in all tests.
Results
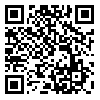
Of the 215 nurses participating in the study, the majority were female (75.8%), aged 30 to 40 years (46%), held a bachelor’s degree in nursing (91.2%), were married (77.7%), had more than 10 years of work experience (35.8%), had a history of COVID-19 (74.9%), and 98% had received the vaccine by the time of the study. The frequency of other demographic characteristics of the participating nurses is presented in Table 1.
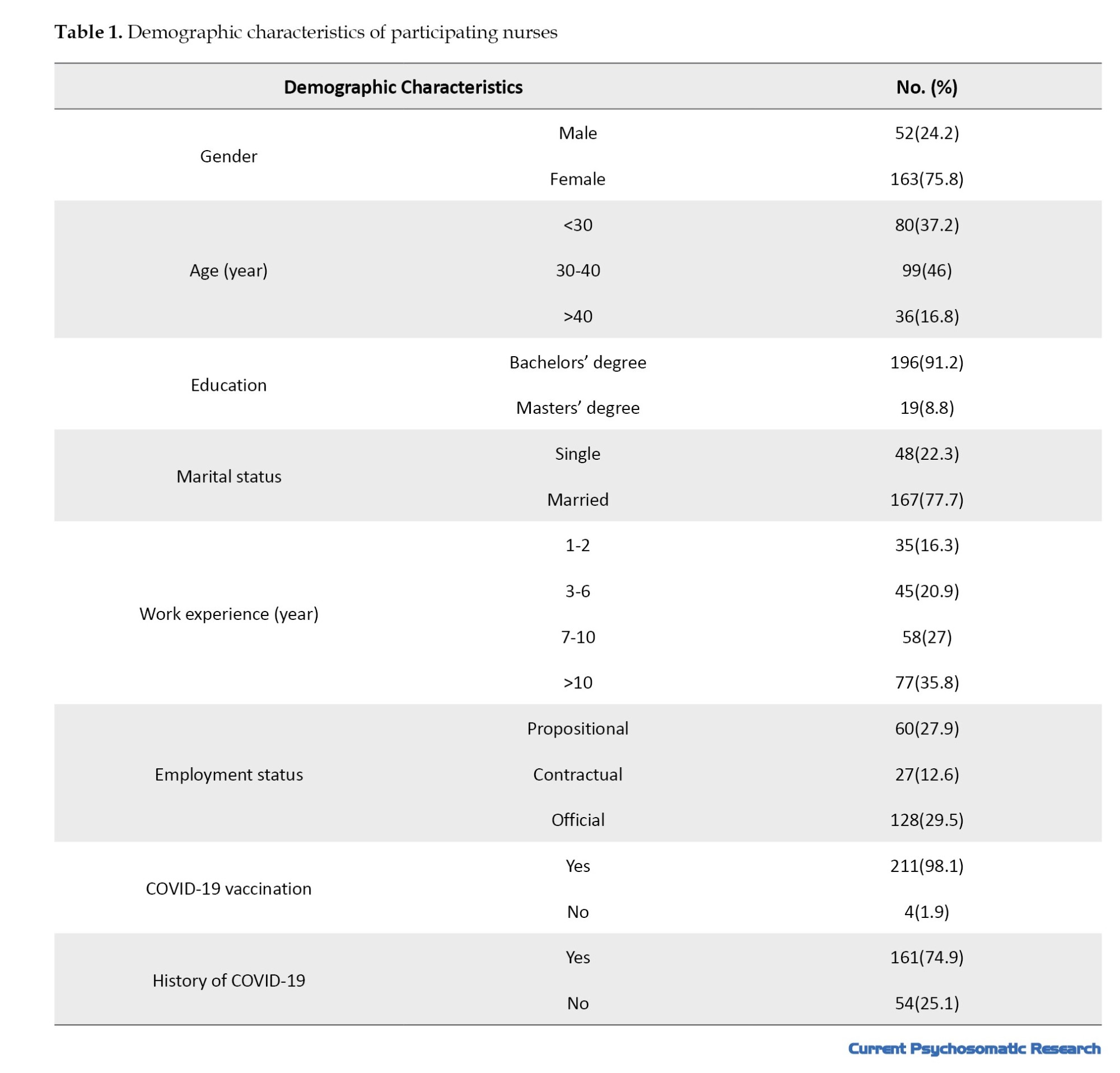
The mean scores for nurses’ resilience and intention to care were 64.77±13.13 and 186.85±31.70, respectively. Table 2 displays the scores of nurses’ resilience and intention to care for COVID-19 patients by dimensions and subcomponents.
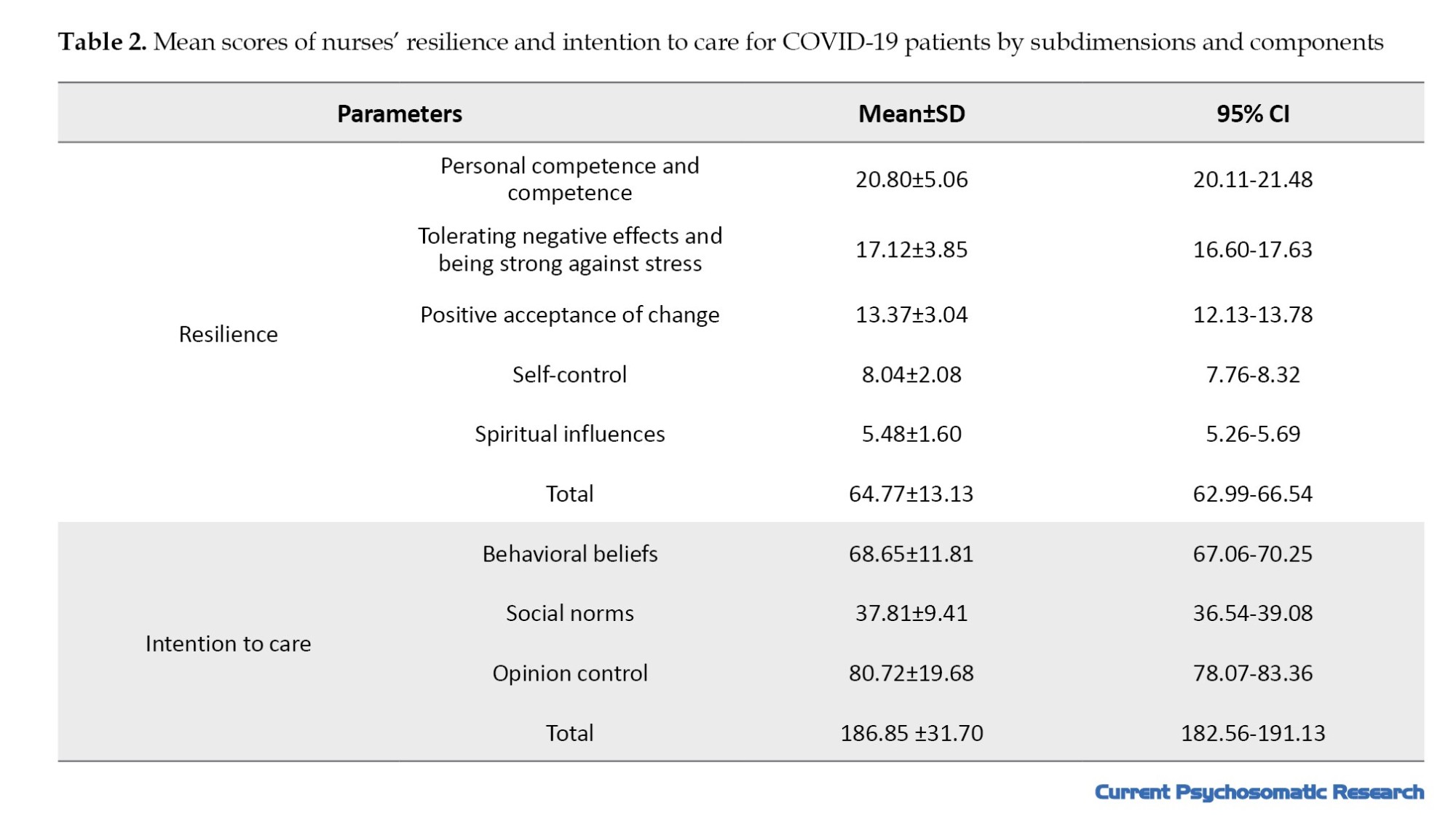
The mean resilience score differed significantly based on “gender” (P=0.001) and “work experience” (P=0.016). Additionally, the difference in the mean score for intention to care for COVID-19 patients was significant only in relation to the “marital status” of the nurses.
To analyze the predictive relationships more precisely, linear regression analysis was performed, revealing that marital status, as the sole demographic variable, significantly predicted intention to care (95% CI, -1.45%, -22.42%; P=0.025; B=-11.44). The coefficient of determination (R²) for this model was 0.02, indicating that marital status explained approximately 2% of the variance in intention to care (Table 3).
The results of the Pearson correlation analysis showed no statistically significant relationship between resilience and intention to care for COVID-19 patients (P=0.567, r=0.039).
Discussion
The aim of this study was to investigate the relationship between nurses’ resilience and their intention to care for COVID-19 patients, as well as the role of certain demographic characteristics in this relationship. The findings indicated that the average resilience score of the participating nurses was 64.77, which is consistent with the results of some previous studies reporting similar levels of resilience among nurses [14, 19].
Although COVID-19 has created numerous challenges for mental health due to fear of illness, fear of death, the spread of false news and rumors, interference with daily activities, travel and movement restrictions, and reduced social relationships (with colleagues, friends, and family), it seems that nurses have utilized resilience during the pandemic as an adaptive mechanism against anxiety, as evidenced by their high average score [20].
The average score of nurses’ intention to care for COVID-19 patients was 186.85. This level of intention is consistent with the findings of several Iranian and international studies, which report moderate intention among nurses [21-23]. In contrast, some studies, particularly in China, have reported higher levels of intention [24, 25]. The increased intention to care among Chinese nurses may be attributed to the salary increases provided by the Chinese government during the pandemic, whereas concerns among nurses in other countries about contracting the virus and potentially spreading COVID-19 to their families may have influenced their intention to care. Providing nurses with adequate information and resources on how to protect themselves could help alleviate fears associated with transmitting COVID-19 to family members [23].
Nurses’ resilience levels based on their demographic characteristics showed a significant difference only in terms of gender and work experience. Specifically, men and personnel with less than two years of work experience or more than ten years reported higher resilience scores. This finding is consistent with the results of Afshari et al. and Barkhordari et al. indicating a significant difference in resilience levels between women and men [14, 26]. The reasons for this difference across various societies can be explained using social role theory, which posits that gender role expectations, skills, and beliefs contribute to behavioral differences between genders [27]. For example, in Iran, a patriarchal society, men are generally expected to exhibit higher social adaptability and resilience than women. While women may possess equal or even higher levels of social adaptability and resilience, they may not feel social pressure to express it outwardly. Iranian women might feel more comfortable discussing their challenges related to adaptability and distress tolerance [28].
Another finding of this study was a statistically significant difference in nurses’ resilience based on their work experience. Similarly, Afshari et al. demonstrated that individuals with more work experience tend to have higher resilience, and there is a significant difference between the various work experience groups in terms of resilience [14]. A higher level of work experience is primarily associated with a better understanding of job stressors and may contribute to the greater resilience of these individuals.
When comparing nurses’ intention to care for COVID-19 patients based on their demographic characteristics, only marital status was statistically significant. Married nurses were 11.44% less likely to care for these patients than single nurses. This finding may be attributed to the family and social roles and responsibilities of married nurses. During a pandemic, concerns about transmitting the virus to family members, particularly spouses and children, can heighten anxiety and stress levels among married nurses, thereby reducing their intention to provide direct care [29, 30]. These results are consistent with those of Tong et al., who found that married Chinese nurses were less willing to care for COVID-19 patients [31]. Al-Hunaishi et al. also reported that factors such as being young, male, and having a higher level of education were associated with an increased intention to work during an epidemic [11]. However, it should be noted that the coefficient of determination in the regression model was low, indicating that marital status could only explain a small portion of the variability in intention to care. Therefore, although this variable was significant, its role is limited, and other factors may also influence nurses’ intention.
Finally, our findings indicate no significant relationship between the level of resilience and the intention of nurses to care for COVID-19 patients. This finding differs from the results of Nantsupawat et al. who showed that nurses with higher resilience reported a lower intention to leave their jobs during the pandemic [13]. During the pandemic, increased levels of job stress among nurses may lead to a decrease in resilience, which could explain the lack of a relationship between resilience and intention to care for COVID-19 patients in the present study [32].
This study, like other cross-sectional studies, had some limitations. For example, its cross-sectional design limits the ability to infer causal relationships. Additionally, the use of convenience sampling may reduce the generalizability of the results. Although the researcher had access to a comprehensive list of nurses, administrative constraints, lack of cooperation from some departments, and the need for rapid data collection during the critical pandemic situation made it impossible to conduct simple random sampling. Furthermore, a significant portion of the information was collected based on the participants’ self-reports, which may be associated with response bias. Conducting the research in a specific city (Amol) may also limit the generalizability of the findings to other regions.
Conclusion
The findings revealed no significant relationship between nurses’ resilience and their intention to care for COVID-19 patients, indicating that resilience could not serve as a predictive factor in this context. Instead, among the demographic characteristics, marital status emerged as the only significant factor, with married nurses being less willing to care for these patients. Additionally, the resilience scores showed a significant difference only based on gender and work experience. These results can assist policymakers and health managers in identifying groups that require more support and in developing targeted programs. It is recommended that future studies examine the role of other psychological and organizational factors, such as social support, burnout, and sense of security, in nurses’ intention to provide care.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1400.309). Verbal informed consent was obtained from all participants. The confidentiality of information and the anonymity of the questionnaires were maintained. Additionally, the 31 codes of the Ethics Committee in Environmental Research of the Ministry of Health were taken into consideration.
Funding
The paper was extracted from the master thesis of Narges Gholipour, approved by Mazandaran University of Medical Sciences, Sari, Iran.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their sincere gratitude to all the nurses who patiently participated in this study by completing the questionnaires, as well as to the colleagues and researchers who provided constructive comments and suggestions that aided us in conducting this research.
References
The COVID-19 pandemic first began in Wuhan, China, in December 2019, and the deadly virus rapidly spread across the globe, quickly becoming a global health crisis [1, 2]. According to the latest report from the World Health Organization (WHO), by the end of July 2024, more than 775 million people worldwide had been infected with the virus, and, unfortunately, over 7 million had died. During the same period, Iran was also affected by this crisis, reporting more than 7.5 million cases and about 147,000 deaths [3]. These alarming statistics highlight the extent and severity of this global crisis.
The widespread infection of COVID-19 within communities poses a unique professional challenge for the healthcare systems of each country. In particular, members of the healthcare team, especially nurses, are on the front lines of the fight against this disease and require significant attention and support [4]. During this crisis, the workload in many hospital departments has increased dramatically, and nurses have been faced with a high volume of patients on a daily basis [5].
The decrease in nurses’ intention to care for COVID-19 patients, especially in crisis situations, could be considered one of the factors affecting the quality of care and the efficiency of the healthcare system. Consequently, identifying the factors that may influence nurses’ intention is an important step toward planning and managing human resources in similar future crises [6].
A nurse’s intention to provide care during a pandemic can be influenced by various individual and organizational factors [7]. Among individual factors, demographic characteristics such as age, gender, marital status, work history, vaccination status, COVID-19 history, and education level have been identified as important variables in predicting nurses’ behavior and their intention to care for patients. For example, Yang et al. and Joseph identified factors such as age and work experience as significant predictors of nurses’ intention to continue working, with more experienced employees demonstrating a greater intention to remain in their roles [8, 9]. Additionally, the study by Kohestani et al. and Al-Hunaishi et al. showed that gender and higher education levels had a significant impact on nurses’ intention to care for COVID-19 patients [10, 11]. These findings highlight the complex interplay of demographic factors influencing nurses’ intention to work in high-risk environments; however, results in this area are not always consistent and can vary based on geographical and cultural contexts.
In addition to demographic characteristics, resilience has also been recognized as an important human ability in coping with occupational stress and health crises. Resilience, defined as the ability to be flexible and return to psychological balance after facing difficult situations, has been identified in numerous studies as a factor that enhances the mental health and professional performance of nurses in critical situations [12]. During the COVID-19 pandemic, resilience has emerged as a key component in maintaining the mental health of nurses. Various studies in different countries have shown that nurses, despite experiencing severe psychological stress, often report moderate to high levels of resilience. For example, a study conducted in Thailand found that high resilience was associated with a reduced tendency to leave the nursing profession [13]. Additionally, research results from Iran indicate that the level of resilience among nurses during different waves of the pandemic was moderate [14, 15].
Recognizing the importance of assessing nurses’ intention to care for patients during the COVID-19 pandemic, as well as the influential role of psychological characteristics like resilience, this study aimed to investigate the relationship between nurses’ resilience and their intention to care for COVID-19 patients. The impact of certain demographic characteristics on this relationship was also analyzed. The results can assist policymakers and health managers in designing and implementing effective programs to support nurses and enhance the quality of health care in critical situations.
Materials and Methods
This descriptive-analytical correlational study was conducted on nurses caring for COVID-19 patients in public hospitals in Amol in 2021. G*Power software, version 3.1 was utilized to ensure an adequate sample size. Considering an effect size of 0.06, a significance level of 0.05, and a test power of 80%, the required sample size was determined to be 215 individuals. The inclusion criteria specified a minimum of 12 months of nursing work experience. This criterion was established to ensure that nurses had sufficient experience in the hospital setting and were familiar with the specific challenges of caring for COVID-19 patients, as indicated by the study conducted by Afshari et al. [14]. This approach will help collect more accurate data and better assess nurses’ intention to care for these patients.
Data were collected using a three-part form. The first part included a demographic checklist that gathered information such as age, gender, marital status, education level, work experience, type of employment, vaccination history, and COVID-19 infection. The second part comprised the Connor–Davidson resilience scale (CD-RISC) [16]. This questionnaire consists of 25 items divided into 5 subscales: Personal competence and efficacy (8 items), tolerance of negative effects and resilience to stress (7 items), positive acceptance of change (5 items), self-control (3 items), and spiritual influences (2 items). The items are scored on a five-point Likert scale as follows: (Completely false=0), (rarely=1), (sometimes true=2), (often true=3), and (always true=4). The highest score an individual can achieve is 100, while the lowest score is zero. A high score on this test indicates a high level of resilience. In this study, the reliability of the instrument was estimated to be 0.914 using Cronbach’s α. The third section included the Nurses’ Intention to Care Scale (NICS), designed by Yoo et al. in 2005 [17]. Responses are scored on a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). This tool is structured into three dimensions: Behavioral beliefs (14 items), social norms (8 items), and belief control (18 items). Test scores range from 40 to 280, with higher scores indicating a greater tendency for nurses to provide higher levels of care. This tool has been psychometrically validated in Persian by Rahmatpour et al. who demonstrated that the factor structure of this instrument accounts for 53.12% of the variance in the concept of intention to care for COVID patients in the Iranian context. Additionally, the values of Cronbach’s α, McDonald’s omega, CR, and maximum reliability of the extracted factors have been reported to exceed 0.8 [18]. In this study, the reliability of the instrument was estimated to be 0.929 using Cronbach’s α.
Procedure
After the research was approved by the Research Council of Mazandaran University of Medical Sciences and received approval from the Ethics Committee, the questionnaires were initially prepared online by uploading them to the Pressline website, and the relevant link was shared in the WhatsApp group for nurses in the target community. However, due to the relatively low participation rate in the online format, the principal investigator, with an official letter of introduction from the university, visited all four hospitals in Amol City—Imam Reza (AS), 17 Shahrivar, Imam Khomeini (RA), and Imam Ali (AS)—which were treating COVID-19 patients at that time. In the in-person format, the researcher physically distributed the questionnaires to volunteer nurses after explaining the study’s objectives. To maintain ethical standards and prevent bias, the questionnaires were completed in a self-administered manner in a separate environment, with the researcher present only for initial guidance and the distribution of the forms. In total, approximately 28% of the sample completed the questionnaires online, while 72% did so in person. Relative quota allocation in the distribution of questionnaires was based on the number of active nurses in the COVID-19 inpatient wards of each hospital.
Data analysis
Data were analyzed using SPSS software, version 26. The normality of data distribution was examined using the Kolmogorov-Smirnov test, which indicated that all main variables followed a normal distribution. Descriptive statistics (Mean±SD, frequency, and percentage) were employed to summarize the data. In the inferential statistics section, an independent t-test and ANOVA were utilized to compare the mean scores of resilience and caregiving tendency between two and multiple groups, respectively. The Pearson correlation test was conducted to examine the relationship between resilience scores and caregiving tendency, while simple linear regression was applied to analyze the predictor variables of intention to care. Additionally, the assumptions of the regression test, including data normality, absence of multicollinearity, and homogeneity of variances, were assessed, and all these assumptions were met. Furthermore, a confidence coefficient of 95% (α=5%), a significance level of 0.05, and a test power of 80% (β=20%) were considered in all tests.
Results
Of the 215 nurses participating in the study, the majority were female (75.8%), aged 30 to 40 years (46%), held a bachelor’s degree in nursing (91.2%), were married (77.7%), had more than 10 years of work experience (35.8%), had a history of COVID-19 (74.9%), and 98% had received the vaccine by the time of the study. The frequency of other demographic characteristics of the participating nurses is presented in Table 1.
The mean scores for nurses’ resilience and intention to care were 64.77±13.13 and 186.85±31.70, respectively. Table 2 displays the scores of nurses’ resilience and intention to care for COVID-19 patients by dimensions and subcomponents.
The mean resilience score differed significantly based on “gender” (P=0.001) and “work experience” (P=0.016). Additionally, the difference in the mean score for intention to care for COVID-19 patients was significant only in relation to the “marital status” of the nurses.
To analyze the predictive relationships more precisely, linear regression analysis was performed, revealing that marital status, as the sole demographic variable, significantly predicted intention to care (95% CI, -1.45%, -22.42%; P=0.025; B=-11.44). The coefficient of determination (R²) for this model was 0.02, indicating that marital status explained approximately 2% of the variance in intention to care (Table 3).
The results of the Pearson correlation analysis showed no statistically significant relationship between resilience and intention to care for COVID-19 patients (P=0.567, r=0.039).
Discussion
The aim of this study was to investigate the relationship between nurses’ resilience and their intention to care for COVID-19 patients, as well as the role of certain demographic characteristics in this relationship. The findings indicated that the average resilience score of the participating nurses was 64.77, which is consistent with the results of some previous studies reporting similar levels of resilience among nurses [14, 19].
Although COVID-19 has created numerous challenges for mental health due to fear of illness, fear of death, the spread of false news and rumors, interference with daily activities, travel and movement restrictions, and reduced social relationships (with colleagues, friends, and family), it seems that nurses have utilized resilience during the pandemic as an adaptive mechanism against anxiety, as evidenced by their high average score [20].
The average score of nurses’ intention to care for COVID-19 patients was 186.85. This level of intention is consistent with the findings of several Iranian and international studies, which report moderate intention among nurses [21-23]. In contrast, some studies, particularly in China, have reported higher levels of intention [24, 25]. The increased intention to care among Chinese nurses may be attributed to the salary increases provided by the Chinese government during the pandemic, whereas concerns among nurses in other countries about contracting the virus and potentially spreading COVID-19 to their families may have influenced their intention to care. Providing nurses with adequate information and resources on how to protect themselves could help alleviate fears associated with transmitting COVID-19 to family members [23].
Nurses’ resilience levels based on their demographic characteristics showed a significant difference only in terms of gender and work experience. Specifically, men and personnel with less than two years of work experience or more than ten years reported higher resilience scores. This finding is consistent with the results of Afshari et al. and Barkhordari et al. indicating a significant difference in resilience levels between women and men [14, 26]. The reasons for this difference across various societies can be explained using social role theory, which posits that gender role expectations, skills, and beliefs contribute to behavioral differences between genders [27]. For example, in Iran, a patriarchal society, men are generally expected to exhibit higher social adaptability and resilience than women. While women may possess equal or even higher levels of social adaptability and resilience, they may not feel social pressure to express it outwardly. Iranian women might feel more comfortable discussing their challenges related to adaptability and distress tolerance [28].
Another finding of this study was a statistically significant difference in nurses’ resilience based on their work experience. Similarly, Afshari et al. demonstrated that individuals with more work experience tend to have higher resilience, and there is a significant difference between the various work experience groups in terms of resilience [14]. A higher level of work experience is primarily associated with a better understanding of job stressors and may contribute to the greater resilience of these individuals.
When comparing nurses’ intention to care for COVID-19 patients based on their demographic characteristics, only marital status was statistically significant. Married nurses were 11.44% less likely to care for these patients than single nurses. This finding may be attributed to the family and social roles and responsibilities of married nurses. During a pandemic, concerns about transmitting the virus to family members, particularly spouses and children, can heighten anxiety and stress levels among married nurses, thereby reducing their intention to provide direct care [29, 30]. These results are consistent with those of Tong et al., who found that married Chinese nurses were less willing to care for COVID-19 patients [31]. Al-Hunaishi et al. also reported that factors such as being young, male, and having a higher level of education were associated with an increased intention to work during an epidemic [11]. However, it should be noted that the coefficient of determination in the regression model was low, indicating that marital status could only explain a small portion of the variability in intention to care. Therefore, although this variable was significant, its role is limited, and other factors may also influence nurses’ intention.
Finally, our findings indicate no significant relationship between the level of resilience and the intention of nurses to care for COVID-19 patients. This finding differs from the results of Nantsupawat et al. who showed that nurses with higher resilience reported a lower intention to leave their jobs during the pandemic [13]. During the pandemic, increased levels of job stress among nurses may lead to a decrease in resilience, which could explain the lack of a relationship between resilience and intention to care for COVID-19 patients in the present study [32].
This study, like other cross-sectional studies, had some limitations. For example, its cross-sectional design limits the ability to infer causal relationships. Additionally, the use of convenience sampling may reduce the generalizability of the results. Although the researcher had access to a comprehensive list of nurses, administrative constraints, lack of cooperation from some departments, and the need for rapid data collection during the critical pandemic situation made it impossible to conduct simple random sampling. Furthermore, a significant portion of the information was collected based on the participants’ self-reports, which may be associated with response bias. Conducting the research in a specific city (Amol) may also limit the generalizability of the findings to other regions.
Conclusion
The findings revealed no significant relationship between nurses’ resilience and their intention to care for COVID-19 patients, indicating that resilience could not serve as a predictive factor in this context. Instead, among the demographic characteristics, marital status emerged as the only significant factor, with married nurses being less willing to care for these patients. Additionally, the resilience scores showed a significant difference only based on gender and work experience. These results can assist policymakers and health managers in identifying groups that require more support and in developing targeted programs. It is recommended that future studies examine the role of other psychological and organizational factors, such as social support, burnout, and sense of security, in nurses’ intention to provide care.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1400.309). Verbal informed consent was obtained from all participants. The confidentiality of information and the anonymity of the questionnaires were maintained. Additionally, the 31 codes of the Ethics Committee in Environmental Research of the Ministry of Health were taken into consideration.
Funding
The paper was extracted from the master thesis of Narges Gholipour, approved by Mazandaran University of Medical Sciences, Sari, Iran.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their sincere gratitude to all the nurses who patiently participated in this study by completing the questionnaires, as well as to the colleagues and researchers who provided constructive comments and suggestions that aided us in conducting this research.
References
- Thompson R. Pandemic potential of 2019-nCoV. Lancet Infect Dis. 2020; 20(3):280. [DOI:10.1016/S1473-3099(20)30068-2] [PMID]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020; 5:536–44. [DOI:10.1038/s41564-020-0695-z]
- World Health Organization (WHO). Coronavirus (COVID-19) Dashboard 2024. 2024 [2026 February 17]. Available from: [Link]
- Turale S, Meechamnan C, Kunaviktikul W. Challenging times: ethics, nursing and the COVID-19 pandemic. Int Nurs Rev. 2020; 67(2):164-7. [DOI:10.1111/inr.12598] [PMID]
- Woo BFY, Lee JXY, Tam WWS. The impact of the advanced practice nursing role on quality of care, clinical outcomes, patient satisfaction, and cost in the emergency and critical care settings: A systematic review. Hum Resour Health. 2017; 15(1):63. [DOI:10.1186/s12960-017-0237-9] [PMID]
- Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. 2020; 3(3):e203976. [DOI:10.1001/jamanetworkopen.2020.3976] [PMID]
- Shrestha GS. COVID-19 pandemic: Shortage of personal protective equipment, use of improvised surrogates, and the safety of health care workers. J Nepal Health Res Counc. 2020; 18(1):150. [DOI:10.33314/jnhrc.v18i1.2593] [PMID]
- Yang PH, Tseng YH, Cheng SC. Exploring significant predictors of retention willingness in nurses diagnosed with COVID-19. Hu Li Za Zhi. 2024; 71(2):58-69. [DOI:10.6224/JN.202404_71(2).08]
- Josef AB, Pascual HG, Surigao AM, Fuentebella J, Calong KC, Soriano GP, et al. Willingness of graduate nursing students to provide care for COVID-19 patients. J Keperawatan Indones. 2023; 26(3):170-9. [DOI:10.7454/jki.v26i3.966]
- Kohestani D, Mohammadinezhad M, Hoseinzadeh E, Sharif Nia H, Shahrabadi S, Aseyedali M. Factors influencing nurses’ intention to care for COVID-19 patients. Curr Psychosom Res. 2022; 1(1):72-83. [DOI:10.32598/cpr.1.1.27.1]
- Al-Hunaishi W, Hoe VC, Chinna K. Factors associated with healthcare workers willingness to participate in disasters: A cross-sectional study in Sana'a, Yemen. BMJ Open. 2019; 9(10):e030547. [DOI:10.1136/bmjopen-2019-030547] [PMID]
- Alameddine M, Clinton M, Bou-Karroum K, Richa N, Doumit MAA. Factors associated with the resilience of nurses during the COVID-19 pandemic. Worldviews Evid Based Nurs. 2021; 18(6):320-31. [DOI:10.1111/wvn.12544] [PMID]
- Nantsupawat A, Kutney-Lee A, Abhicharttibutra K, Wichaikhum OA, Poghosyan L. Exploring the relationships between resilience, burnout, work engagement, and intention to leave among nurses in the context of the COVID-19 pandemic: A cross-sectional study. BMC Nurs. 2024; 23(1):290. [DOI:10.1186/s12912-024-01958-1] [PMID]
- Afshari D, Nourollahi-Darabad M, Chinisaz N. Demographic predictors of resilience among nurses during the COVID-19 pandemic. Work. 2021; 68(2):297-303. [DOI:10.3233/WOR-203376] [PMID]
- Parizad N, Soheili A, Powers K, Mohebbi I, Moghbeli G, Hosseingolipour K. Level of resilience in nurses working at COVID-19 referral centers in Iran. Nurs Forum. 2022; 57(3):344-51. [DOI:10.1111/nuf.12685] [PMID]
- Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76-82. [DOI:10.1002/da.10113] [PMID]
- Yoo HR, Kwon BE, Jang YS, Youn HK. [Validity and reliability of an instrument for predictive nursing intention for SARS patient care (Korean)]. Taehan Kanho Hakhoe Chi. 2005; 35(6):1063-71 [DOI:10.4040/jkan.2005.35.6.1063] [PMID]
- Rahmatpour P, Sharif Nia H, Sivarajan Froelicher E, Kaveh O, Pahlevan Sharif S, Taghipour B. Psychometric evaluation of Persian version of nurses' intention to care scale (P-NICS) for patients with COVID-19. Int J Gen Med. 2020; 13:515-22. [DOI:10.2147/IJGM.S260579] [PMID]
- Sotoodeh A, Rahmani-Anaraki H, Sabzi Z. [Evaluation of resilience and its relationship with some individual professional factors of nurses working in the intensive care unit (ICU) of hospitals affiliated to Golestan University of Medical Sciences 2020 (Persian)]. Nurs Dev Health. 2021; 11(2):36-43. [Link]
- Li ZS, Hasson F. Resilience, stress, and psychological well-being in nursing students: A systematic review. Nurse Educ Today. 2020; 90:104440. [DOI:10.1016/j.nedt.2020.104440] [PMID]
- Zarei s, kazemi a. [The moderating effect of perceived organizational support and psychological resiliency in the relationship between job stress with job productivity among nurses (Persian)]. Iran J Nurs Res. 2020; 15(2):45-57. [Link]
- Lord H, Loveday C, Moxham L, Fernandez R. Effective communication is key to intensive care nurses' willingness to provide nursing care amidst the COVID-19 pandemic. Intensive Crit Care Nurs. 2021; 62:102946. [DOI:10.1016/j.iccn.2020.102946] [PMID]
- Nashwan AJ, Abujaber AA, Mohamed AS, Villar RC, Al-Jabry MM. Nurses' willingness to work with COVID-19 patients: The role of knowledge and attitude. Nurs Open. 2021; 8(2):695-701. [DOI:10.1002/nop2.674] [PMID]
- Yu Y, Yu Y, Hu J. COVID-19 among Chinese high school graduates: Psychological distress, growth, meaning in life and resilience. J Health Psychol. 2022; 27(5):1057-69. [DOI:10.1177/1359105321990819] [PMID]
- Wu B, Zhao Y, Xu D, Wang Y, Niu N, Zhang M, et al. Factors associated with nurses' willingness to participate in care of patients with COVID-19: A survey in China. J Nurs Manag. 2020; 28(7):1704-12. [DOI:10.1111/jonm.13126] [PMID]
- Barkhordari-Sharifabad M, Hekayati M, Nasiriani K. [The Relationship between Moral Distress and Resiliency in Nurses (Persian)]. Med Ethic J. 2020; 13(45):1-14. [Link]
- Eagly AH, Wood W. The nature-nurture debates: 25 years of challenges in understanding the psychology of gender. Perspect Psychol Sci. 2013; 8(3):340-57. [DOI:10.4324/9780203781906] [PMID]
- Falavarjani MF, Yeh CJ. Optimism and distress tolerance in the social adjustment of nurses: Examining resilience as a mediator and gender as a moderator. J Res Nurs. 2019; 24(7):500-12. [DOI:10.1177/1744987119839102] [PMID]
- Labrague LJ, de Los Santos JAA. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J Nurs Manag. 2021; 29(3):395-403. [DOI:10.1111/jonm.13168] [PMID]
- Charney RL, Rebmann T, Flood RG. Hospital employee willingness to work during earthquakes versus pandemics. J Emerg Med. 2015; 49(5):665-74. [DOI:10.1016/j.jemermed.2015.07.030] [PMID]
- Tong LK, Zhu MX, Wang SC, Cheong PL, Van IK. Nurses Who Are More Willing to Participate in the Fight against COVID-19: Evidence from China. Int J Environ Res Public Health. 2021; 18(14):7357. [DOI:10.3390/ijerph18147357] [PMID]
- Mahdieh O, Darvishi GS. [The study of the relationship b etween nurses’job stress and resiliency (Persian)]. J Nurse Phys Within War. 2017. [Link]
Type of Study: Research |
Subject:
Psychiatric Nursing
Received: 2025/06/25 | Accepted: 2024/08/10 | Published: 2024/10/1
Received: 2025/06/25 | Accepted: 2024/08/10 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
