Wed, May 27, 2026
[Archive]
Volume 3, Issue 1 (Autumn 2024)
CPR 2024, 3(1): 53-62 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rezapour M, Karami H, Naderi Sorki M, Shabanpour S. Investigating the Relationship Between Parathyroid Hormone Levels and Depression and Anxiety in Patients With Transfusion-dependent Thalassemia. CPR 2024; 3 (1) :53-62
URL: http://cpr.mazums.ac.ir/article-1-126-en.html
URL: http://cpr.mazums.ac.ir/article-1-126-en.html



Psychiatric and Behavioral Sciences Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Mazandaran, Iran.
Full-Text [PDF 728 kb]
(32 Downloads)
| Abstract (HTML) (94 Views)
Full-Text: (14 Views)
Introduction
Thalassemia is a hereditary blood disorder characterized by reduced hemoglobin production, leading to mild-to-severe anemia [1]. Mutations in the beta-globin gene result in inappropriate synthesis of the beta-globin protein, leading to an imbalance between the alpha and beta-globin chains. Free alpha chains accumulate in red blood cells, leading to beta-thalassemia [2].
Thalassemia syndrome is classified based on clinical manifestations and the need for blood transfusions. Inappropriate hemoglobin production results in ineffective erythropoiesis and increased peripheral hemolysis [3]. Iron overload resulting from repeated transfusions causes complications and mortality in transfusion-dependent patients.
Excess iron is often deposited in the liver, heart, and endocrine system [3, 4]. In patients with transfusion-dependent thalassemia (TDT), frequent blood transfusions and iron overload lead to numerous endocrine complications, including hypogonadism, diabetes, hypothyroidism, and hypoparathyroidism [5].
Following iron deposition in the parathyroid glands, thalassemia patients become susceptible to hypoparathyroidism. Parathyroid hormone (PTH) is a polypeptide hormone secreted by the parathyroid gland [6]. Hypoparathyroidism is a hormonal disorder resulting from the absence or reduced blood level of PTH. Hypoparathyroidism leads to hypocalcemia, hyperphosphatemia, and hypercalciuria [7].
The reported prevalence of hypoparathyroidism in patients with TDT ranges from 4% to 40% [8]. Hypoparathyroidism affects various body systems, including the kidneys, nerves, psyche, skeleton, and immune system, with neuropsychiatric complications being among the most significant [9, 10].
The rate of neuropsychiatric complications, including depression, has been reported to be higher in patients with non-surgical hypoparathyroidism than in healthy individuals [11].
Approximately 320,000 children are born annually with hemoglobinopathies, and nearly 80% of these births occur in developing countries [12]. Patients with thalassemia are exposed to psychological consequences that affect disease progression and both short- and long-term outcomes [13].
Depression and anxiety are prevalent in thalassemia patients, with their prevalence significantly higher than in the general population. Studies have shown that up to 80% of patients with thalassemia may experience some degree of mental disorders. Psychosocial factors, such as recurrent hospitalizations, comorbidities (such as diabetes and heart failure), short stature, and delayed puberty, are among the most significant predictors of these disorders [14, 15].
In patients with thalassemia, disturbances in calcium, phosphorus, Vitamin D, and PTH metabolism are very common. Vitamin D deficiency, hypocalcemia, hyperphosphatemia, and elevated PTH occur due to chronic iron loading, liver damage, and endocrine disorders. These disturbances lead to decreased bone mineral density and an increased risk of fracture. Iron overload and liver damage play key roles in these disturbances, and their severity increases with age and disease severity [16, 17].
There is substantial evidence linking Vitamin D deficiency to increased depression and anxiety in both the general population and patients with thalassemia. Vitamin D acts as a neurosteroid that regulates brain function and mood, and its deficiency is associated with increased symptoms of depression and anxiety. Furthermore, elevated PTH has been associated with cognitive impairment and depression [18, 19]; studies have indicated that individuals with higher PTH levels have poorer cognitive function and higher depression scores. Calcium and phosphorus disturbances can also affect mental health and sleep quality; specifically, hypocalcemia and phosphorus abnormalities are associated with increased anxiety and sleep disturbances [19, 20].
Despite numerous studies in this area, the direct relationship between PTH levels and depression and anxiety in these patients has been less explored. Identifying this relationship can lead to a better understanding of the biological mechanisms affecting psychiatric disorders and aid in designing more targeted therapeutic interventions. Therefore, this study aimed to investigate the relationship between PTH levels and depression and anxiety in patients with thalassemia to contribute to integrated biological and psychological interventions for these patients.
Materials and Methods
Study design and setting
This analytical cross-sectional study included patients with TDT who were actively referred to the Thalassemia Ward of Bou-Ali Hospital in Sari City, Mazandaran Province, Iran, for blood transfusions at least once monthly in 2023.
Sample size calculation
The standard formula (Equation 1) for comparing the means of two independent groups was utilized to calculate the required sample size. The parameters employed in this formula were identical to those used in a previous study [21]:
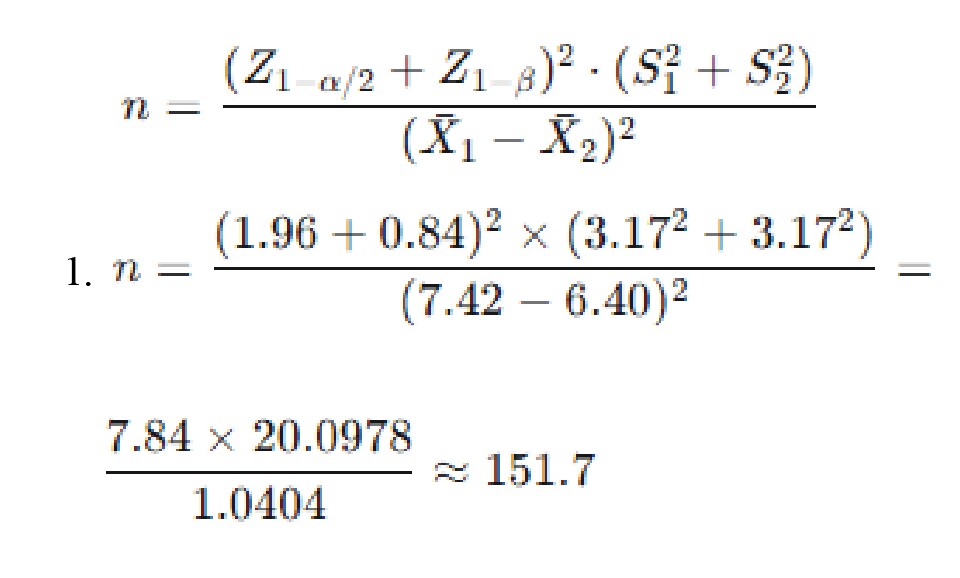
Considering the possibility of incomplete or missing responses, a 20% attrition rate was assumed, leading to a preliminary final sample size of 190 individuals. To enhance precision and patient accessibility, the final sample size for the current study was set at 204 participants, exceeding the minimum required.
Inclusion and exclusion criteria
The inclusion criteria were as follows:
1) Diagnosis of TDT; 2) Age e 18; 3) Absence of any severe emotional stressor within the preceding three months (e.g. fatal accident, bereavement, or divorce); 4) Absence of severe comorbidities, including pulmonary hypertension, liver or kidney failure, chronic diseases such as cancer, significant cognitive impairment, mental retardation, or current substance use (drugs or stimulants).
The exclusion criteria were as follows:
Incomplete medical records lacking the data required for this study; 2) refusal to provide informed consent for participation; and 3) failure to undergo the required laboratory assessments for serum levels of PTH, calcium, phosphorus, and vitamin D.
Data collection and assessment tools
Information regarding the use of psychotropic medications, tobacco (cigarettes), and alcohol was systematically recorded. After written informed consent was obtained, a comprehensive demographic questionnaire was administered. This questionnaire collected data on: age, gender, marital status, presence of other physical comorbidities, history of psychiatric illness, current psychiatric medication use, annual frequency of hospital visits, and status of PTH, calcium, phosphorus, and Vitamin D levels, as well as the total number of blood transfusions received.
Psychiatric symptoms were evaluated using the hospital anxiety and depression scale (HADS). All necessary laboratory tests were conducted free of charge at the Bou-Ali Hospital Laboratory, utilizing identical methods and equipment for standardization.
The HADS questionnaire consists of 14 items, divided into two independent subscales: anxiety and depression. Each item was scored on a scale of 0-3. The total score for each subscale ranged from 0 to 21. The following thresholds were used to categorize the severity for both the anxiety and depression subscales:
Normal: ≤7; Mild: 8−10; Modeate: 11−14; Severe: 5−21
The validity and reliability of the HADS in the Iranian population have been previously confirmed, with reported Cronbach’s α values of 0.78 for anxiety and 0.86 for depression [22]. The questionnaires were self-administered by the patients under the direct supervision of the research student.
Grouping based on HADS scores
The completed HADS questionnaires allowed for the division of patients into two main categories: depressed vs. non-depressed, and anxious vs non-anxious. Patients scoring ≤7 were categorized as non-depressed, while those scoring >7 were categorized based on their score into mild, moderate, or severe depression. Similarly, patients with scores ≤7 were grouped as non-anxious, while those with scores >7 were categorized into mild, moderate, or severe anxiety groups. The measured levels of PTH, Vitamin D, calcium, and phosphorus for all patients were recorded from their files and subsequently compared and analyzed.
Statistical analysis
After the study was completed, the data were compiled. Statistical analyses and interpretations were then performed using STATA software, version 13. Descriptive statistics, such as Mean±SD, were used if the primary outcome demonstrated a normal distribution; otherwise, the median and interquartile range (IQR) were employed.
In addition to comparing the serum levels of PTH, Vitamin D, calcium, and phosphorus between patients with depression/anxiety and those without, the percentage of patients with hypoparathyroidism was compared between these two groups. Simple linear regression was used to examine the association between depression/anxiety and PTH. The independent t-test and analysis of variance were employed for group mean comparisons, and multiple linear regression was used to control for potential confounding variables.
Results
Based on Table 1, the mean age of the participants in our study was 36.13±6.17 years. Of the 204 patients examined, 107 (52.5%) were female. The number of married individuals (126; 61.8%), was higher than that of single and divorced individuals. Furthermore, 58 participants (28.4%) had an education level below a diploma, and 146 participants (71.6%) had diplomas or higher.
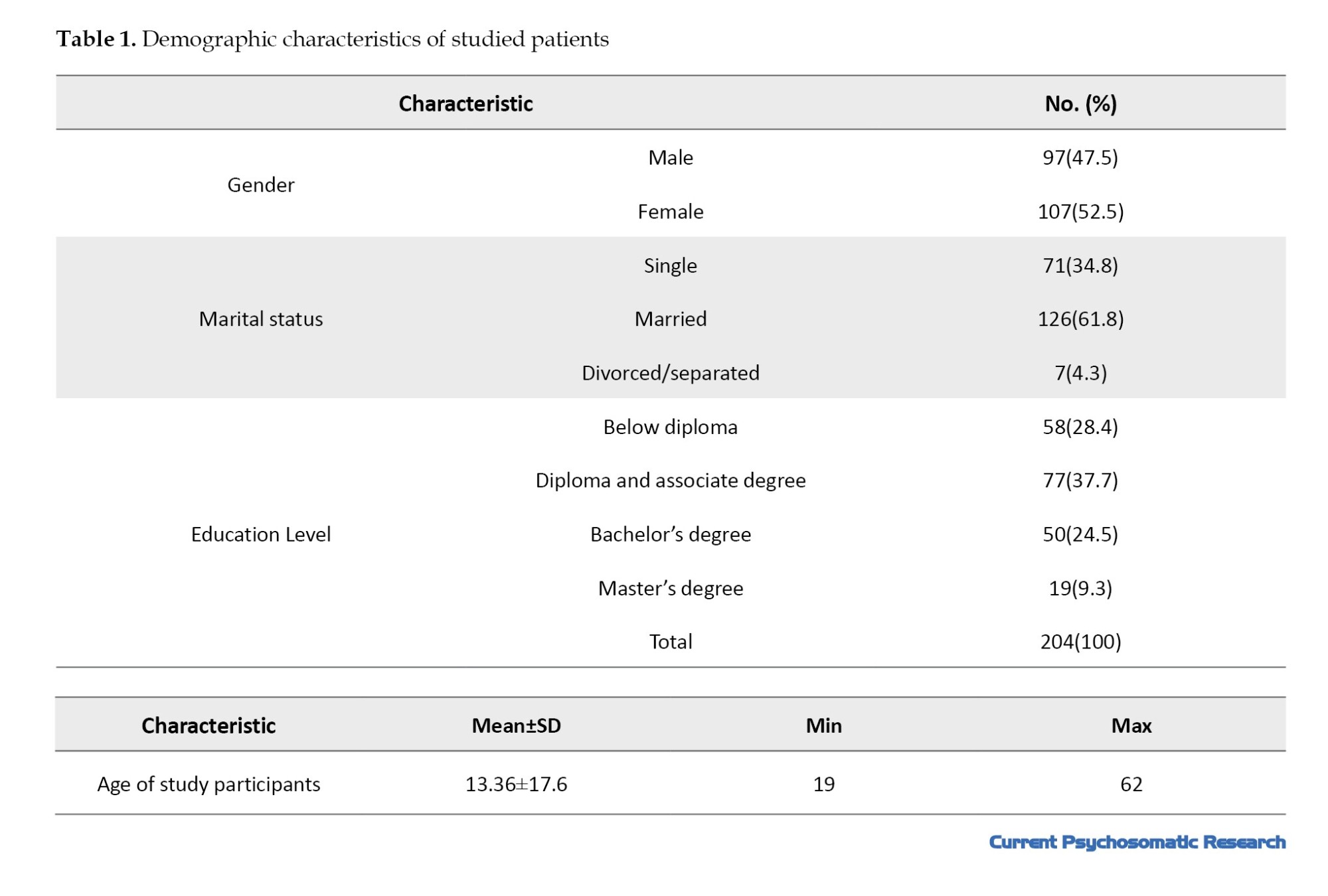
Additionally, among the study participants, 32 individuals (15.84% of the 204 participants) reported a history of smoking. Only six individuals mentioned alcohol consumption.
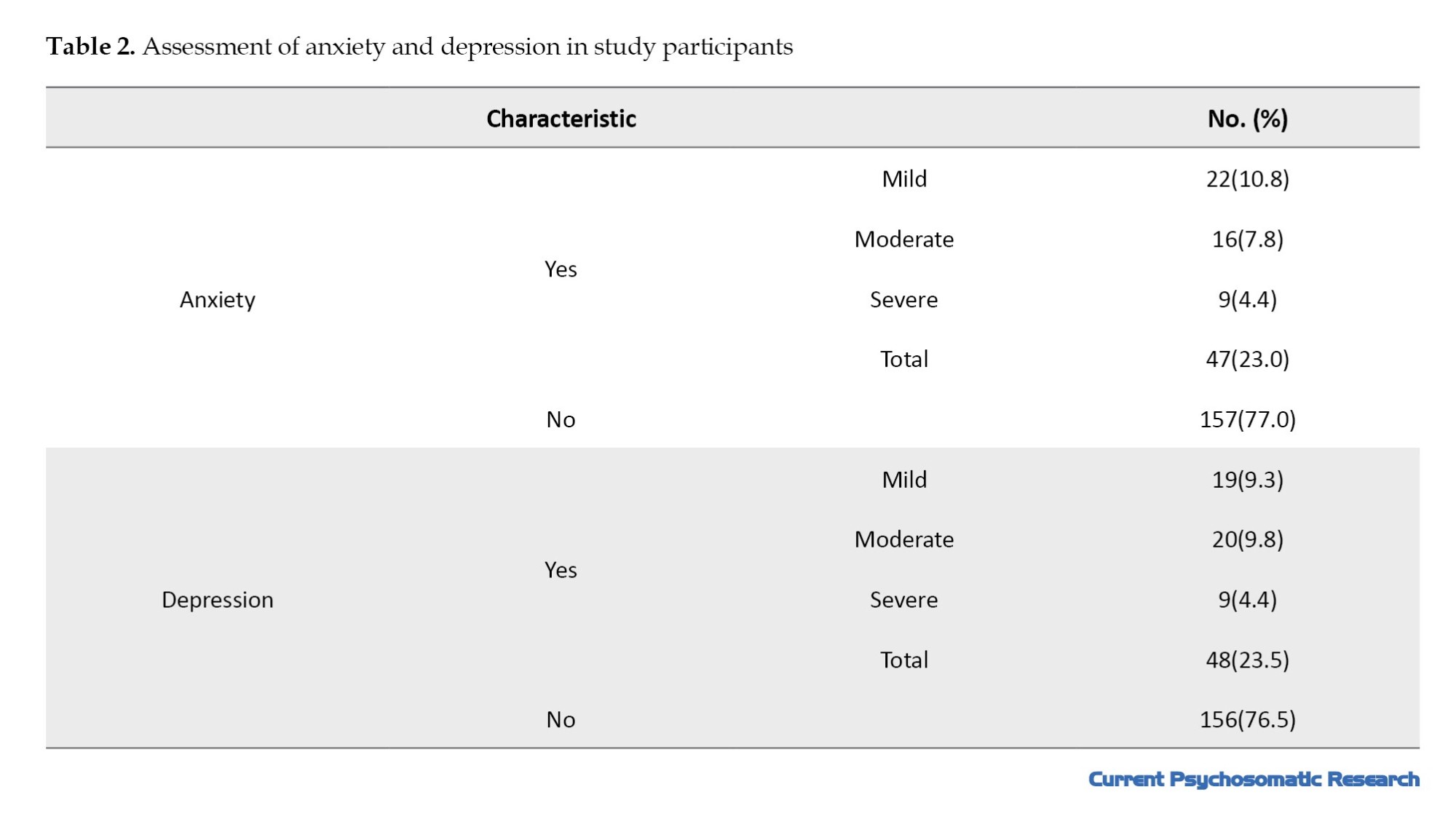
According to Table 2, in our study, 47 individuals (23.0%) experienced anxiety, of whom only 9 (4.4%) reported severe anxiety, and 22 (10.8%) reported mild anxiety. The prevalence of depression in the studied sample was 48 individuals (23.5%), where, similar to anxiety, 9 (4.4%) had severe depression, 19 (9.3%) had mild depression, and the remainder had moderate depression. The mean anxiety score was 50.5±4.25, with the highest score being 19. The mean depression score in the sample was low at 40.7±4.60.
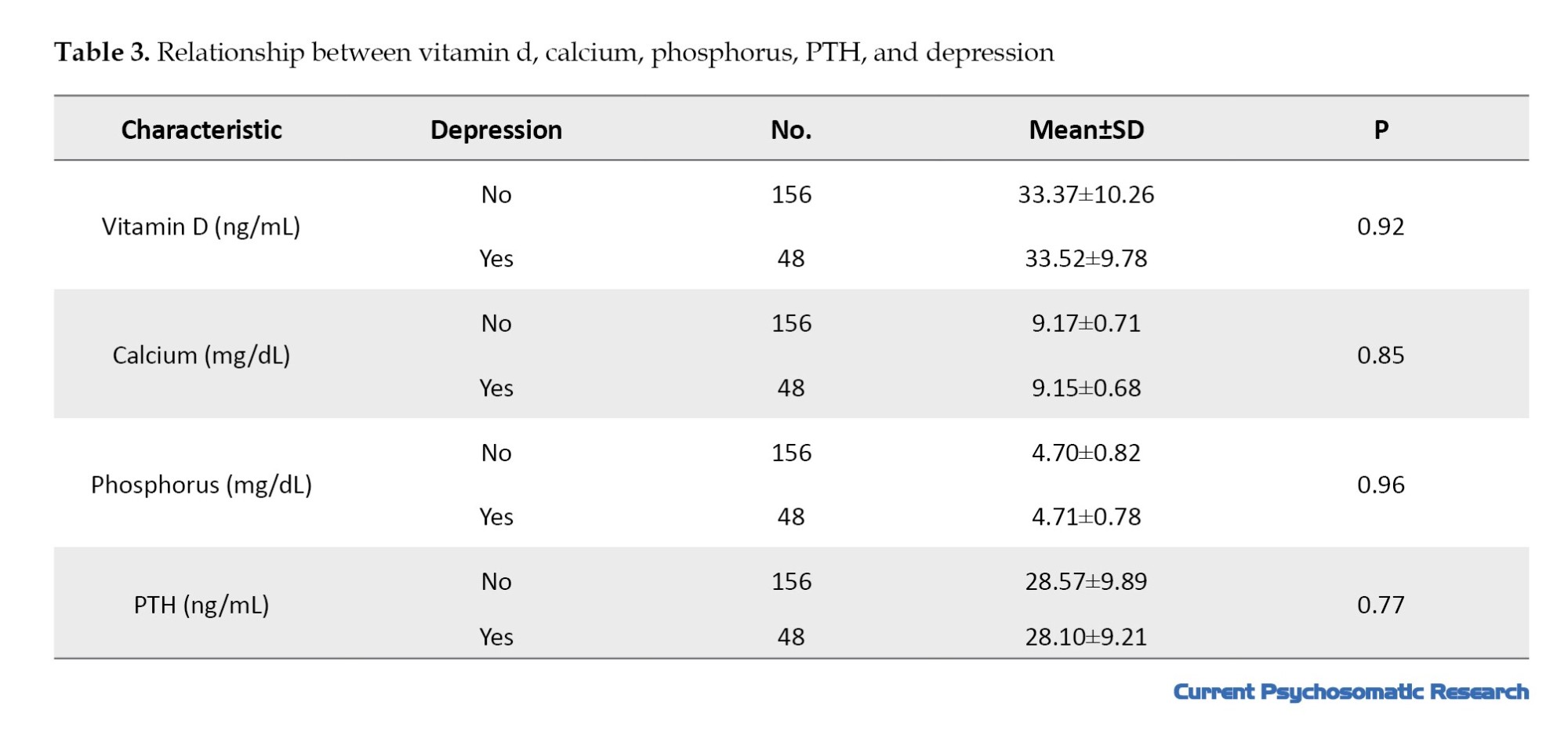
Based on Table 3, the mean level of Vitamin D was 33.40±10.12 ng/mL, and the mean level of PTH in the study was 28.46±9.71 ng/mL. The minimum and maximum PTH values were 1.2 and 41 ng/mL, respectively.
Individuals were divided into two groups: those with and those without depression, and the mean levels of Vitamin D, calcium, phosphorus, and PTH were examined. None of the four factors under consideration showed a statistically significant difference with depression (P=0.92, P=0.85, P=0.96, P=0.77).
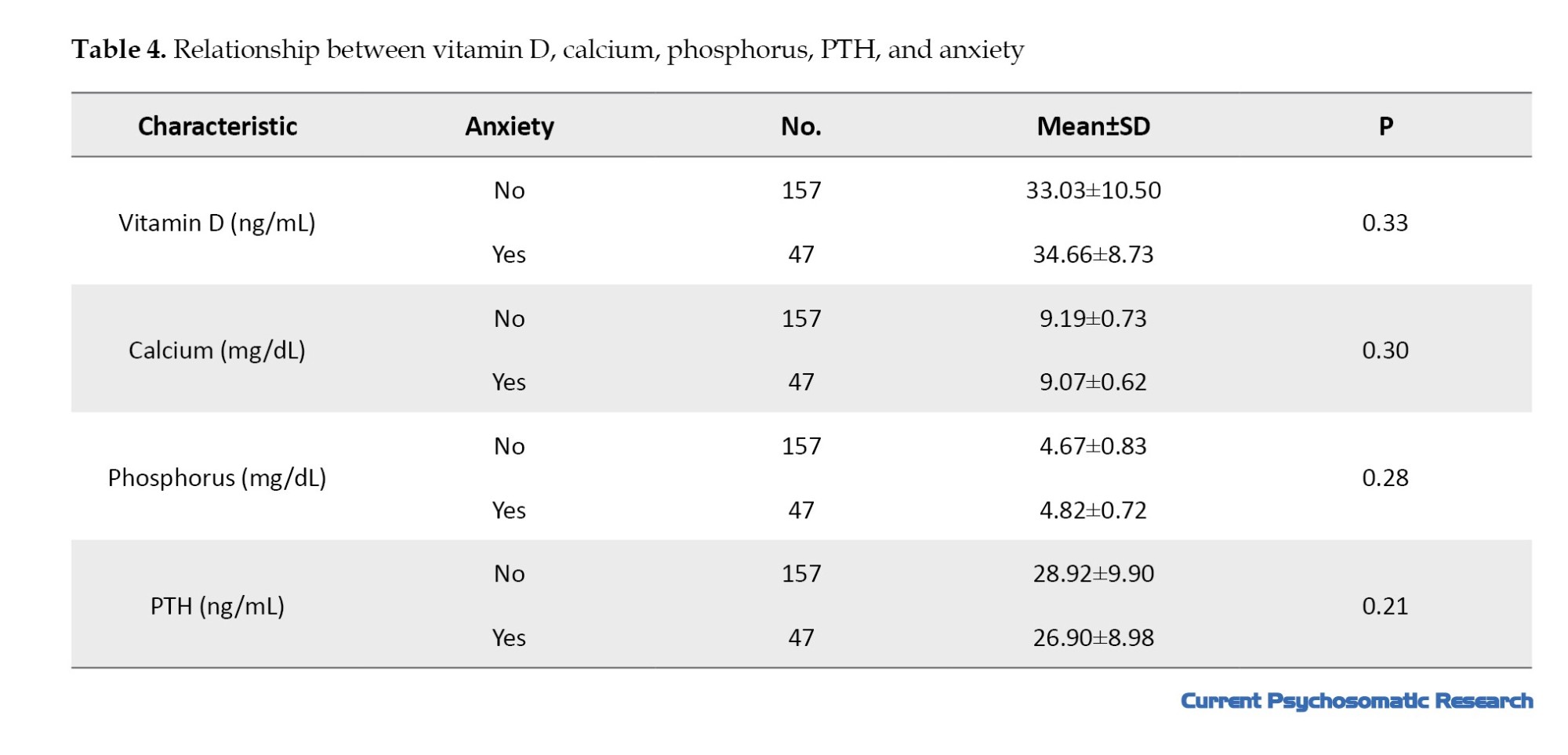
Based on Table 4, in the investigation of the relationship between the mean levels of Vitamin D, Calcium, Phosphorus, and PTH and anxiety, no significant differences were found between anxiety and the variables under consideration (P=0.33, P=0.30, P=0.28, P=0.21).
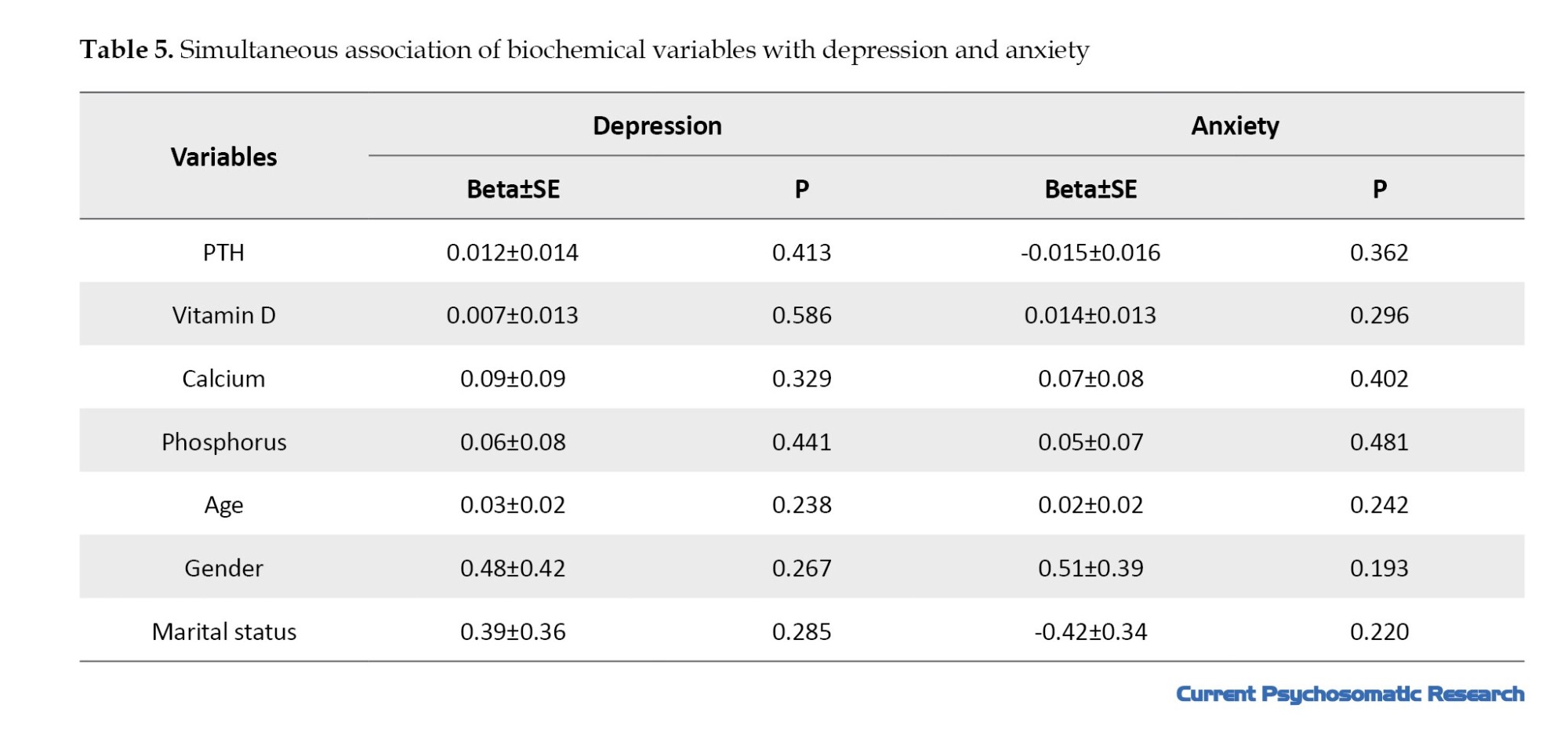
To simultaneously investigate the effects of biochemical and demographic variables, two multiple regression models were used to predict the depression and anxiety scores.
According to Table 5, based on the multiple regression results, none of the variables—Vitamin D, Calcium, Phosphorus, age, gender, or marital status—showed a significant association with either depression or anxiety.
The Beta coefficients and R2 values were 0.06 for depression and 0.05 for anxiety. These values indicate that the evaluated variables play a small role in explaining the variance of depression and anxiety. Beta represents the regression coefficient, and SE represents the standard error.
Discussion
Patients with thalassemia are exposed to psychological consequences that affect the course of the disease and its short- and long-term outcomes [13].
Based on various studies, the prevalence of psychiatric disorders in patients with thalassemia is reported to be between 25% and 30% [12]. Hypoparathyroidism is a complication of blood transfusions in patients with TDT. According to existing studies, hypoparathyroidism can lead to the onset of neuropsychiatric symptoms, including depression. Given the high prevalence of psychiatric disorders in patients with thalassemia and the significant role of biopsychosocial factors in the development of psychiatric symptoms, this study aimed to investigate the relationship between the level of PTH, which is a crucial biological factor, and depression and anxiety in patients with TDT.
In the present study, depressive symptoms were observed in 23% of the patients, with moderate and severe depression reported in 15% of the patients. This is a significantly lower percentage than that reported by Zolaly et al. [23]. Zolaly’s study involved 62 patients and used the Depression, Anxiety and Stress Scale-21 Items (DASS-21) assessment tool; the smaller sample size and different assessment tool may account for the difference in results. Notably, our findings are consistent with the prevalence reported internationally [24–26]. In the analysis performed, patients with thalassemia did not show very high anxiety scores. The mean scores for both sections of the questionnaire (5.50 in the anxiety section and 4.70 in the depression section) were less than 7, indicating normality (individuals scoring below 7 were considered normal, and those scoring above 7 were considered anxious or depressed). However, there were notably severe cases in the study, with the highest anxiety and depression scores being 19 out of 21.
Anxiety was diagnosed in 23.5% of our patients, with severe anxiety in approximately 4.4% and moderate anxiety in 7.8% [23]. Several studies have reported the prevalence of depression in patients with thalassemia, varying from 10% to 50%, with our study reporting this figure at 23.5% [21, 27, 28].
Various reports from Iran indicate that depression in thalassemia patients is a dominant manifestation, ranging between 12% and 30%, with up to 54% of patients suffering from some form of pathological mental disorder [23, 29, 30]. More serious psychological complications can occur in patients with thalassemia. One study in Iran reported that up to 27.3% of patients had contemplated suicide in the year preceding the study [31]. In Arab societies, a 2012 study reported similar findings in 80 patients in Lebanon, where 35% of the patients were depressed [32]. Al-Hakeim et al. reported that severe depression in children with thalassemia is strongly associated with the number of blood transfusions, iron overload, and increased levels of interleukin-1β [33]. In Saudi Arabia, a study on patients with sickle cell anemia in the Qatif region reported that 48% of the patients had depressive symptoms. This may suggest that all patients with hereditary hemoglobinopathies or other chronic medical diagnoses are at risk of developing mental disorders [34]. Adolescents with chronic medical diagnoses, such as thalassemia, are at higher risk for psychological disorders, such as identity problems and hormonal changes. However, children and older patients remain at risk for serious stress-related psychiatric and mental disorders associated with stress [21].
Hypoparathyroidism is well-recognized among blood transfusion-dependent β-thalassemia patients and is often observed in patients with higher iron stores, frequently accompanied by other endocrine disorders [35–37]. Acquired hypoparathyroidism resulting from hemosiderosis (due to repeated blood transfusions) is always the first consideration for hypocalcemia in patients with thalassemia. However, ferritin concentration is not a reliable predictor of hypoparathyroidism because many studies have reported no significant difference in serum ferritin levels between patients with and without hypoparathyroidism [38–40]. This study investigated the mean serum levels of Vitamin D, calcium, phosphorus, and PTH in relation to depression and anxiety.
A comparison of serum levels of Vitamin D, calcium, phosphorus, and PTH between depressed and non-depressed patients showed that none of the biochemical variables correlated significantly with depression (P=0.92, P=0.85, P=0.96, and P=0.77, respectively).
In examining the relationship of the above indicators with anxiety, no significant difference was observed between the two groups. The values were P=0.33 for Vitamin D, P=0.30 for calcium, P=0.28 for phosphorus, and P=0.21 for PTH.
To simultaneously investigate the effect of biochemical and demographic variables, two multiple regression models were used to predict the depression and anxiety scores. Based on the results of the multiple regressions, none of the variables—Vitamin D, calcium, phosphorus, age, gender, or marital status—showed a statistically significant association with either depression or anxiety.
The Beta coefficients and R2 values were 0.06 for depression and 0.05 for anxiety. These values indicate that the evaluated variables explain very little variance in depression and anxiety. Regression assumptions, including normality of residuals, lack of multicollinearity (VIF <2), independence of errors, and homogeneity of variance, were checked and confirmed. Accordingly, the regression models were statistically valid, but their predictive power was weak.
The findings of this study contradict some previous studies that reported an association between high PTH or low Vitamin D levels and depression and anxiety. Based on this, the role of psychosocial factors and the burden and complications of chronic disease contribute more significantly than biological factors. The choice of assessment tools, sample size, disease severity, and other confounding factors may lead to these differing results.
Early diagnosis and appropriate support and management are highly needed to help patients cope with the illness and improve their quality of life. All patients with symptoms of depression, anxiety, or stress should be referred to a psychiatric clinic for appropriate intervention. Further studies with a long follow-up program and multi-center national registration are highly needed to optimize the appropriate care for these patients. Considering that the instruments for assessing depression and anxiety differ across various studies, different results are expected, and a semi-structured psychiatric interview may yield more comparable results. It is also recommended that future research utilize longitudinal studies and larger patient cohorts to establish a clearer causal relationship.
Conclusion
Despite prior studies suggesting a correlation between PTH levels and depression, this study found no significant association between the mean serum levels of vitamin D, calcium, phosphorus, or PTH and depression or anxiety in patients with TDT.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1402.11700).
Funding
This article is extracted from the General Practitioner dissertation of Soheil Shabanpour, approved by Mazandaran University of Medical Sciences, Sari, Iran.
Authors' contributions
Writing the manuscript: Maryam Rezapour and Soheil Shabanpour; Study design: Maryam Rezapour; Research: Hossein Karami; Data analysis: Mohammad Naderi Sorki; Data collection: Soheil Shabanpour.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The research team expresses its sincere gratitude to the thalassemia patients and the esteemed personnel of the Thalassemia Ward at Bou-Ali Hospital, Sari City, for their cooperation in conducting this study.
References
Thalassemia is a hereditary blood disorder characterized by reduced hemoglobin production, leading to mild-to-severe anemia [1]. Mutations in the beta-globin gene result in inappropriate synthesis of the beta-globin protein, leading to an imbalance between the alpha and beta-globin chains. Free alpha chains accumulate in red blood cells, leading to beta-thalassemia [2].
Thalassemia syndrome is classified based on clinical manifestations and the need for blood transfusions. Inappropriate hemoglobin production results in ineffective erythropoiesis and increased peripheral hemolysis [3]. Iron overload resulting from repeated transfusions causes complications and mortality in transfusion-dependent patients.
Excess iron is often deposited in the liver, heart, and endocrine system [3, 4]. In patients with transfusion-dependent thalassemia (TDT), frequent blood transfusions and iron overload lead to numerous endocrine complications, including hypogonadism, diabetes, hypothyroidism, and hypoparathyroidism [5].
Following iron deposition in the parathyroid glands, thalassemia patients become susceptible to hypoparathyroidism. Parathyroid hormone (PTH) is a polypeptide hormone secreted by the parathyroid gland [6]. Hypoparathyroidism is a hormonal disorder resulting from the absence or reduced blood level of PTH. Hypoparathyroidism leads to hypocalcemia, hyperphosphatemia, and hypercalciuria [7].
The reported prevalence of hypoparathyroidism in patients with TDT ranges from 4% to 40% [8]. Hypoparathyroidism affects various body systems, including the kidneys, nerves, psyche, skeleton, and immune system, with neuropsychiatric complications being among the most significant [9, 10].
The rate of neuropsychiatric complications, including depression, has been reported to be higher in patients with non-surgical hypoparathyroidism than in healthy individuals [11].
Approximately 320,000 children are born annually with hemoglobinopathies, and nearly 80% of these births occur in developing countries [12]. Patients with thalassemia are exposed to psychological consequences that affect disease progression and both short- and long-term outcomes [13].
Depression and anxiety are prevalent in thalassemia patients, with their prevalence significantly higher than in the general population. Studies have shown that up to 80% of patients with thalassemia may experience some degree of mental disorders. Psychosocial factors, such as recurrent hospitalizations, comorbidities (such as diabetes and heart failure), short stature, and delayed puberty, are among the most significant predictors of these disorders [14, 15].
In patients with thalassemia, disturbances in calcium, phosphorus, Vitamin D, and PTH metabolism are very common. Vitamin D deficiency, hypocalcemia, hyperphosphatemia, and elevated PTH occur due to chronic iron loading, liver damage, and endocrine disorders. These disturbances lead to decreased bone mineral density and an increased risk of fracture. Iron overload and liver damage play key roles in these disturbances, and their severity increases with age and disease severity [16, 17].
There is substantial evidence linking Vitamin D deficiency to increased depression and anxiety in both the general population and patients with thalassemia. Vitamin D acts as a neurosteroid that regulates brain function and mood, and its deficiency is associated with increased symptoms of depression and anxiety. Furthermore, elevated PTH has been associated with cognitive impairment and depression [18, 19]; studies have indicated that individuals with higher PTH levels have poorer cognitive function and higher depression scores. Calcium and phosphorus disturbances can also affect mental health and sleep quality; specifically, hypocalcemia and phosphorus abnormalities are associated with increased anxiety and sleep disturbances [19, 20].
Despite numerous studies in this area, the direct relationship between PTH levels and depression and anxiety in these patients has been less explored. Identifying this relationship can lead to a better understanding of the biological mechanisms affecting psychiatric disorders and aid in designing more targeted therapeutic interventions. Therefore, this study aimed to investigate the relationship between PTH levels and depression and anxiety in patients with thalassemia to contribute to integrated biological and psychological interventions for these patients.
Materials and Methods
Study design and setting
This analytical cross-sectional study included patients with TDT who were actively referred to the Thalassemia Ward of Bou-Ali Hospital in Sari City, Mazandaran Province, Iran, for blood transfusions at least once monthly in 2023.
Sample size calculation
The standard formula (Equation 1) for comparing the means of two independent groups was utilized to calculate the required sample size. The parameters employed in this formula were identical to those used in a previous study [21]:
Considering the possibility of incomplete or missing responses, a 20% attrition rate was assumed, leading to a preliminary final sample size of 190 individuals. To enhance precision and patient accessibility, the final sample size for the current study was set at 204 participants, exceeding the minimum required.
Inclusion and exclusion criteria
The inclusion criteria were as follows:
1) Diagnosis of TDT; 2) Age e 18; 3) Absence of any severe emotional stressor within the preceding three months (e.g. fatal accident, bereavement, or divorce); 4) Absence of severe comorbidities, including pulmonary hypertension, liver or kidney failure, chronic diseases such as cancer, significant cognitive impairment, mental retardation, or current substance use (drugs or stimulants).
The exclusion criteria were as follows:
Incomplete medical records lacking the data required for this study; 2) refusal to provide informed consent for participation; and 3) failure to undergo the required laboratory assessments for serum levels of PTH, calcium, phosphorus, and vitamin D.
Data collection and assessment tools
Information regarding the use of psychotropic medications, tobacco (cigarettes), and alcohol was systematically recorded. After written informed consent was obtained, a comprehensive demographic questionnaire was administered. This questionnaire collected data on: age, gender, marital status, presence of other physical comorbidities, history of psychiatric illness, current psychiatric medication use, annual frequency of hospital visits, and status of PTH, calcium, phosphorus, and Vitamin D levels, as well as the total number of blood transfusions received.
Psychiatric symptoms were evaluated using the hospital anxiety and depression scale (HADS). All necessary laboratory tests were conducted free of charge at the Bou-Ali Hospital Laboratory, utilizing identical methods and equipment for standardization.
The HADS questionnaire consists of 14 items, divided into two independent subscales: anxiety and depression. Each item was scored on a scale of 0-3. The total score for each subscale ranged from 0 to 21. The following thresholds were used to categorize the severity for both the anxiety and depression subscales:
Normal: ≤7; Mild: 8−10; Modeate: 11−14; Severe: 5−21
The validity and reliability of the HADS in the Iranian population have been previously confirmed, with reported Cronbach’s α values of 0.78 for anxiety and 0.86 for depression [22]. The questionnaires were self-administered by the patients under the direct supervision of the research student.
Grouping based on HADS scores
The completed HADS questionnaires allowed for the division of patients into two main categories: depressed vs. non-depressed, and anxious vs non-anxious. Patients scoring ≤7 were categorized as non-depressed, while those scoring >7 were categorized based on their score into mild, moderate, or severe depression. Similarly, patients with scores ≤7 were grouped as non-anxious, while those with scores >7 were categorized into mild, moderate, or severe anxiety groups. The measured levels of PTH, Vitamin D, calcium, and phosphorus for all patients were recorded from their files and subsequently compared and analyzed.
Statistical analysis
After the study was completed, the data were compiled. Statistical analyses and interpretations were then performed using STATA software, version 13. Descriptive statistics, such as Mean±SD, were used if the primary outcome demonstrated a normal distribution; otherwise, the median and interquartile range (IQR) were employed.
In addition to comparing the serum levels of PTH, Vitamin D, calcium, and phosphorus between patients with depression/anxiety and those without, the percentage of patients with hypoparathyroidism was compared between these two groups. Simple linear regression was used to examine the association between depression/anxiety and PTH. The independent t-test and analysis of variance were employed for group mean comparisons, and multiple linear regression was used to control for potential confounding variables.
Results
Based on Table 1, the mean age of the participants in our study was 36.13±6.17 years. Of the 204 patients examined, 107 (52.5%) were female. The number of married individuals (126; 61.8%), was higher than that of single and divorced individuals. Furthermore, 58 participants (28.4%) had an education level below a diploma, and 146 participants (71.6%) had diplomas or higher.
Additionally, among the study participants, 32 individuals (15.84% of the 204 participants) reported a history of smoking. Only six individuals mentioned alcohol consumption.
According to Table 2, in our study, 47 individuals (23.0%) experienced anxiety, of whom only 9 (4.4%) reported severe anxiety, and 22 (10.8%) reported mild anxiety. The prevalence of depression in the studied sample was 48 individuals (23.5%), where, similar to anxiety, 9 (4.4%) had severe depression, 19 (9.3%) had mild depression, and the remainder had moderate depression. The mean anxiety score was 50.5±4.25, with the highest score being 19. The mean depression score in the sample was low at 40.7±4.60.
Based on Table 3, the mean level of Vitamin D was 33.40±10.12 ng/mL, and the mean level of PTH in the study was 28.46±9.71 ng/mL. The minimum and maximum PTH values were 1.2 and 41 ng/mL, respectively.
Individuals were divided into two groups: those with and those without depression, and the mean levels of Vitamin D, calcium, phosphorus, and PTH were examined. None of the four factors under consideration showed a statistically significant difference with depression (P=0.92, P=0.85, P=0.96, P=0.77).
Based on Table 4, in the investigation of the relationship between the mean levels of Vitamin D, Calcium, Phosphorus, and PTH and anxiety, no significant differences were found between anxiety and the variables under consideration (P=0.33, P=0.30, P=0.28, P=0.21).
To simultaneously investigate the effects of biochemical and demographic variables, two multiple regression models were used to predict the depression and anxiety scores.
According to Table 5, based on the multiple regression results, none of the variables—Vitamin D, Calcium, Phosphorus, age, gender, or marital status—showed a significant association with either depression or anxiety.
The Beta coefficients and R2 values were 0.06 for depression and 0.05 for anxiety. These values indicate that the evaluated variables play a small role in explaining the variance of depression and anxiety. Beta represents the regression coefficient, and SE represents the standard error.
Discussion
Patients with thalassemia are exposed to psychological consequences that affect the course of the disease and its short- and long-term outcomes [13].
Based on various studies, the prevalence of psychiatric disorders in patients with thalassemia is reported to be between 25% and 30% [12]. Hypoparathyroidism is a complication of blood transfusions in patients with TDT. According to existing studies, hypoparathyroidism can lead to the onset of neuropsychiatric symptoms, including depression. Given the high prevalence of psychiatric disorders in patients with thalassemia and the significant role of biopsychosocial factors in the development of psychiatric symptoms, this study aimed to investigate the relationship between the level of PTH, which is a crucial biological factor, and depression and anxiety in patients with TDT.
In the present study, depressive symptoms were observed in 23% of the patients, with moderate and severe depression reported in 15% of the patients. This is a significantly lower percentage than that reported by Zolaly et al. [23]. Zolaly’s study involved 62 patients and used the Depression, Anxiety and Stress Scale-21 Items (DASS-21) assessment tool; the smaller sample size and different assessment tool may account for the difference in results. Notably, our findings are consistent with the prevalence reported internationally [24–26]. In the analysis performed, patients with thalassemia did not show very high anxiety scores. The mean scores for both sections of the questionnaire (5.50 in the anxiety section and 4.70 in the depression section) were less than 7, indicating normality (individuals scoring below 7 were considered normal, and those scoring above 7 were considered anxious or depressed). However, there were notably severe cases in the study, with the highest anxiety and depression scores being 19 out of 21.
Anxiety was diagnosed in 23.5% of our patients, with severe anxiety in approximately 4.4% and moderate anxiety in 7.8% [23]. Several studies have reported the prevalence of depression in patients with thalassemia, varying from 10% to 50%, with our study reporting this figure at 23.5% [21, 27, 28].
Various reports from Iran indicate that depression in thalassemia patients is a dominant manifestation, ranging between 12% and 30%, with up to 54% of patients suffering from some form of pathological mental disorder [23, 29, 30]. More serious psychological complications can occur in patients with thalassemia. One study in Iran reported that up to 27.3% of patients had contemplated suicide in the year preceding the study [31]. In Arab societies, a 2012 study reported similar findings in 80 patients in Lebanon, where 35% of the patients were depressed [32]. Al-Hakeim et al. reported that severe depression in children with thalassemia is strongly associated with the number of blood transfusions, iron overload, and increased levels of interleukin-1β [33]. In Saudi Arabia, a study on patients with sickle cell anemia in the Qatif region reported that 48% of the patients had depressive symptoms. This may suggest that all patients with hereditary hemoglobinopathies or other chronic medical diagnoses are at risk of developing mental disorders [34]. Adolescents with chronic medical diagnoses, such as thalassemia, are at higher risk for psychological disorders, such as identity problems and hormonal changes. However, children and older patients remain at risk for serious stress-related psychiatric and mental disorders associated with stress [21].
Hypoparathyroidism is well-recognized among blood transfusion-dependent β-thalassemia patients and is often observed in patients with higher iron stores, frequently accompanied by other endocrine disorders [35–37]. Acquired hypoparathyroidism resulting from hemosiderosis (due to repeated blood transfusions) is always the first consideration for hypocalcemia in patients with thalassemia. However, ferritin concentration is not a reliable predictor of hypoparathyroidism because many studies have reported no significant difference in serum ferritin levels between patients with and without hypoparathyroidism [38–40]. This study investigated the mean serum levels of Vitamin D, calcium, phosphorus, and PTH in relation to depression and anxiety.
A comparison of serum levels of Vitamin D, calcium, phosphorus, and PTH between depressed and non-depressed patients showed that none of the biochemical variables correlated significantly with depression (P=0.92, P=0.85, P=0.96, and P=0.77, respectively).
In examining the relationship of the above indicators with anxiety, no significant difference was observed between the two groups. The values were P=0.33 for Vitamin D, P=0.30 for calcium, P=0.28 for phosphorus, and P=0.21 for PTH.
To simultaneously investigate the effect of biochemical and demographic variables, two multiple regression models were used to predict the depression and anxiety scores. Based on the results of the multiple regressions, none of the variables—Vitamin D, calcium, phosphorus, age, gender, or marital status—showed a statistically significant association with either depression or anxiety.
The Beta coefficients and R2 values were 0.06 for depression and 0.05 for anxiety. These values indicate that the evaluated variables explain very little variance in depression and anxiety. Regression assumptions, including normality of residuals, lack of multicollinearity (VIF <2), independence of errors, and homogeneity of variance, were checked and confirmed. Accordingly, the regression models were statistically valid, but their predictive power was weak.
The findings of this study contradict some previous studies that reported an association between high PTH or low Vitamin D levels and depression and anxiety. Based on this, the role of psychosocial factors and the burden and complications of chronic disease contribute more significantly than biological factors. The choice of assessment tools, sample size, disease severity, and other confounding factors may lead to these differing results.
Early diagnosis and appropriate support and management are highly needed to help patients cope with the illness and improve their quality of life. All patients with symptoms of depression, anxiety, or stress should be referred to a psychiatric clinic for appropriate intervention. Further studies with a long follow-up program and multi-center national registration are highly needed to optimize the appropriate care for these patients. Considering that the instruments for assessing depression and anxiety differ across various studies, different results are expected, and a semi-structured psychiatric interview may yield more comparable results. It is also recommended that future research utilize longitudinal studies and larger patient cohorts to establish a clearer causal relationship.
Conclusion
Despite prior studies suggesting a correlation between PTH levels and depression, this study found no significant association between the mean serum levels of vitamin D, calcium, phosphorus, or PTH and depression or anxiety in patients with TDT.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1402.11700).
Funding
This article is extracted from the General Practitioner dissertation of Soheil Shabanpour, approved by Mazandaran University of Medical Sciences, Sari, Iran.
Authors' contributions
Writing the manuscript: Maryam Rezapour and Soheil Shabanpour; Study design: Maryam Rezapour; Research: Hossein Karami; Data analysis: Mohammad Naderi Sorki; Data collection: Soheil Shabanpour.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The research team expresses its sincere gratitude to the thalassemia patients and the esteemed personnel of the Thalassemia Ward at Bou-Ali Hospital, Sari City, for their cooperation in conducting this study.
References
- Oliveros O, Trachtenberg F, Haines D, Gerstenberger E, Martin M, Carson S, et al. Pain over time and its effects on life in thalassemia. Am J Hematol. 2013; 88(11):939-43. [DOI:10.1002/ajh.23565] [PMID]
- Motta I, Mancarella M, Marcon A, Vicenzi M, Cappellini MD. Management of age-associated medical complications in patients with β-thalassemia. Expert Rev Hematol. 2020; 13(1):85-94. [DOI:10.1080/17474086.2020.1686354] [PMID]
- Majumder A, Basu S. Hypoparathyroidism in a Case of Transfusion Dependent Thalassemia. J ASEAN Fed EndocrSoc. 2020; 35(1):129-32. [DOI:10.15605/jafes.035.01.23] [PMID]
- Bordbar M, Omrani GR, Haghpanah S, Saki F, Karimi M, Zekavat O. Bone mineral density in transfusion-dependent thalassemia patients and its associated factors in Southern Iran. Arch Osteoporos. 2020; 15(1):148. [DOI:10.1007/s11657-020-00811-7] [PMID]
- Saki F, Salehifar A, Kassaee SR, Omrani GR. Association of vitamin D and FGF23 with serum ferritin in hypoparathyroid thalassemia: A case control study. BMC Nephrol. 2020; 21(1):482. [DOI:10.1186/s12882-020-02101-3] [PMID]
- Azami M, Parizad N, Sayehmiri K. Prevalence of hypothyroidism, hypoparathyroidism and the frequency of regular chelation therapy in patients with thalassemia major in Iran: A systematic review and meta-analysis study. Iran J Ped Hematol Oncol. 2016; 6(4):261-76. [Link]
- Munkongdee T, Chen P, Winichagoon P, Fucharoen S, Paiboonsukwong K. Update in laboratory diagnosis of thalassemia. Front Mol Biosci. 2020; 7:74. [DOI:10.3389/fmolb.2020.00074] [PMID]
- Tangngam H, Mahachoklertwattana P, Poomthavorn P, Chuansumrit A, Sirachainan N, Chailurkit L, et al. Under-recognized hypoparathyroidism in thalassemia. J Clin Res Pediatr Endocrinol. 2018; 10(4):324-30. [DOI:10.4274/jcrpe.0020] [PMID]
- Cusano NE, Bilezikian JP. Signs and symptoms of hypoparathyroidism. Endocrinol Metab Clin North Am. 2018; 47(4):759-70. [DOI:10.1016/j.ecl.2018.07.001] [PMID]
- Gaba S, Singla M, Gupta M, Dua A, Gaba N. From Psychiatry to Neurology and Endocrinology: A Case of Hypoparathyroidism. Cureus. 2020; 12(9):e10666. [DOI:10.7759/cureus.10666]
- Underbjerg L, Sikjaer T, Mosekilde L, Rejnmark L. The epidemiology of nonsurgical hypoparathyroidism in Denmark: A nationwide case finding study. J Bone Miner Res. 2015; 30(9):1738-44. [DOI:10.1002/jbmr.2501] [PMID]
- Nisha S, Alam SS, Rahman MN, Islam K. A Strategy to Assess Morbidity Pattern, Mental Health of Patients with Thalassemia: Physiological and Mental Health Conditions. Am J Med Case Rep. 2021; 9(1):4-8. [DOI:10.12691/ajmcr-9-1-2]
- Zolaly MA, Zolaly FM, Al Belowi L, Shuqdar R, Al Belowi Sr MA, Alwasaidi TA, et al. Depression, Anxiety, and Stress Symptoms in Patients With Beta Thalassemia Major in Almadinah Almunawwarah, Saudi Arabia. Cureus. 2020; 12(11):e11367. [DOI:10.7759/cureus.11367] [PMID]
- Yahia S, El-Hadidy MA, El-Gilany AH, Anwar R, Darwish A, Mansour A. Predictors of anxiety and depression in Egyptian thalassemic patients: A single center study. Int J Hematol. 2013; 97(5):604-9. [DOI:10.1007/s12185-013-1322-z] [PMID]
- Mednick L, Yu S, Trachtenberg F, Xu Y, Kleinert DA, Giardina PJ, et al. Symptoms of depression and anxiety in patients with thalassemia: Prevalence and correlates in the thalassemia longitudinal cohort. Am J Hematol Oncol. 2010; 85(10):802-5. [DOI:10.1002/ajh.21826] [PMID]
- Manolopoulos P, Lavranos G, Mamais I, Angouridis A, Giannakou K, Johnson E. Vitamin D and bone health status in beta thalassemia patients-systematic review. Osteoporos Int. 2021; 32(6):1031-40. [DOI:10.1007/s00198-021-05821-w] [PMID]
- Napoli N, Carmina E, Bucchieri S, Sferrazza C, Rini G, Di Fede G. Low serum levels of 25-hydroxy vitamin D in adults affected by thalassemia major or intermedia. Bone. 2006; 38(6):888-92. [DOI:10.1016/j.bone.2005.11.018] [PMID]
- Silva MRM, Barros WMA, Silva MLD, Silva JMLD, Souza APDS, Silva ABJD, et al. Relationship between vitamin D deficiency and psychophysiological variables: A systematic review of the literature. Clinics. 2021; 76:e3155. [DOI:10.6061/clinics/2021/e3155] [PMID]
- Jorde R, Waterloo K, Saleh F, Haug E, Svartberg J. Neuropsychological function in relation to serum parathyroid hormone and serum 25-hydroxyvitamin D levels: The Tromsø study. J Neurol. 2006; 253(4):464-70. [DOI:10.1007/s00415-005-0027-5] [PMID]
- Hoogendijk WJ, Lips P, Dik MG, Deeg DJ, Beekman AT, Penninx BW. Depression is associated with decreased 25-hydroxyvitamin D and increased parathyroid hormone levels in older adults. Arch Gen Psychiatry. 2008; 65(5):508-12. [DOI:10.1001/archpsyc.65.5.508] [PMID]
- Maheri A, Sadeghi R, Shojaeizadeh D, Tol A, Yaseri M, Rohban A. Depression, Anxiety, and Perceived Social Support among Adults with Beta-Thalassemia Major: Cross-Sectional Study. Korean J Fam Med. 2018; 39(2):101-7. [DOI:10.4082/kjfm.2018.39.2.101] [PMID]
- Kaviani H, Seyfourian H, Sharifi V, Ebrahimkhani N. Reliability and validity of anxiety and depression hospital scales (HADS): Iranian patients with anxiety and depression disorders. Tehran Univ Med J. 2009; 67(5):379-85. [Link]
- Zolaly MA, Zolaly FM, Al Belowi L, Shuqdar R, Al Belowi MA Sr, Alwasaidi TA, et al. Depression, Anxiety, and Stress Symptoms in Patients With Beta Thalassemia Major in Almadinah Almunawwarah, Saudi Arabia. Cureus. 2020; 12(11):e11367. [DOI:10.7759/cureus.11367] [PMID]
- Habeb AM, Al-Hawsawi ZM, Morsy MM, Al-Harbi AM, Osilan AS, Al-Magamsi MS, et al. Endocrinopathies in beta-thalassemia major. Prevalence, risk factors, and age at diagnosis in Northwest Saudi Arabia. Saudi Med J. 2013; 34(1):67-73. [DOI:10.15537/1658-3175.5693] [PMID]
- Al-Zahrani A. Factors structure and the psychometric characteristics of depression, anxiety, and stress scale (DASS-21) in Saudi environment. Iraqi Acad Sci J. 2019; 2019:626-40. [Link]
- Antony MM, Bieling PJ, Cox BJ, Enns MW, Swinson R. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychological Assessment. 1998; 10(2):176–81. [DOI:10.1037/1040-3590.10.2.176]
- Mednick L, Yu S, Trachtenberg F, Xu Y, Kleinert DA, Giardina PJ, et al. Symptoms of depression and anxiety in patients with thalassemia: Prevalence and correlates in the thalassemia longitudinal cohort. Am J Hematol. 2010; 85(10):802-5. [DOI:10.1002/ajh.21826] [PMID]
- Koutelekos J, Haliasos N. Depression and Thalassemia in children, adolescents and adults. Health Sci J. 2013; 7(3):239-46. [Link]
- Naderi M, Hormozi MR, Ashrafi M, Emamdadi A. Evaluation of Mental Health and Related Factors among Patients with Beta-thalassemia Major in South East of Iran. Iran J Psychiatry. 2012; 7(1):47-51. [PMID]
- Behdani F, Badiee Z, Hebrani P, Moharreri F, Badiee AH, Hajivosugh N, et al. Psychological Aspects in Children and Adolescents With Major Thalassemia: A Case-Control Study. Iran J Pediatr. 2015; 25(3):e322. [DOI:10.5812/ijp.322] [PMID]
- Ghanizadeh A, Khajavian S, Ashkani H. Prevalence of psychiatric disorders, depression, and suicidal behavior in child and adolescent with thalassemia major. J Pediatr Hematol Oncol. 2006; 28(12):781-4. [DOI:10.1097/01.mph.0000243665.79303.9e] [PMID]
- Khoury B, Musallam KM, Abi-Habib R, Bazzi L, Ward ZA, Succar J, et al. Prevalence of depression and anxiety in adult patients with β-thalassemia major and intermedia. Int J Psychiatry Med. 2012; 44(4):291-303. [DOI:10.2190/PM.44.4.a] [PMID]
- Al-Hakeim HK, Najm AH, Al-Aldujaili AH, Maes M. Major depression in children with β-thalassemia major is strongly associated with the number of blood transfusions, iron overload and increased levels of interleukin-1β. 2019. Preprints. [DOI:10.20944/preprints201909.0033.v1]
- Alhomoud MA, Gosadi IM, Wahbi HA. Depression among Sickle Cell Anemia Patients in the Eastern Province of Saudi Arabia. Saudi J Med Med Sci. 2018; 6(1):8-12. [DOI:10.4103/sjmms.sjmms_123_16] [PMID]
- De Sanctis V, Vullo C, Bagni B, Chiccoli L. Hypoparathyroidism in beta-thalassemia major. Clinical and laboratory observations in 24 patients. Acta Haematol. 1992; 88(2-3):105-8. [DOI:10.1159/000204662] [PMID]
- Gabriele OF. Hypoparathyroidism associate with thalassemia. South Med J. 1971; 64(1):115-6. [DOI:10.1097/00007611-197101000-00025] [PMID]
- Chern JP, Lin KH. Hypoparathyroidism in transfusion-dependent patients with beta-thalassemia. J Pediatr Hematol Oncol. 2002; 24(4):291-3. [DOI:10.1097/00043426-200205000-00014] [PMID]
- Angelopoulos NG, Goula A, Rombopoulos G, Kaltzidou V, Katounda E, Kaltsas D, et al. Hypoparathyroidism in transfusion-dependent patients with beta-thalassemia. J Bone Miner Metab. 2006; 24(2):138-45. [DOI:10.1007/s00774-005-0660-1] [PMID]
- Chern JP, Lin KH, Tsai WY, Wang SC, Lu MY, Lin DT, et al. Hypogonadotropic hypogonadism and hematologic phenotype in patients with transfusion-dependent beta-thalassemia. J Pediatr Hematol Oncol. 2003; 25(11):880-4. [DOI:10.1097/00043426-200311000-00011] [PMID]
- Filosa A, Di Maio S, Vocca S, Saviano A, Esposito G, Pagano L. Longitudinal monitoring of bone mineral density in thalassemic patients. Genetic structure and osteoporosis. Acta Paediatr. 1997; 86(4):342-6. [DOI:10.1111/j.1651-2227.1997.tb09019.x] [PMID]
Type of Study: Research |
Subject:
Psychology
Received: 2024/06/6 | Accepted: 2024/08/26 | Published: 2024/10/1
Received: 2024/06/6 | Accepted: 2024/08/26 | Published: 2024/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
