Wed, May 27, 2026
[Archive]
Volume 2, Issue 2 (Winter 2024)
CPR 2024, 2(2): 113-122 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Toghani F, Mirzaian B, Zaboli E, Amini F. Effectiveness of Cognitive-behavioral Stress Management on the Quality of Life of Women With Breast Cancer in Sari. CPR 2024; 2 (2) :113-122
URL: http://cpr.mazums.ac.ir/article-1-101-en.html
URL: http://cpr.mazums.ac.ir/article-1-101-en.html



Department of Clinical Psychology, Faculty of Medicine, Sari Branch, Islamic Azad University, Sari, Iran.
Keywords: Cognitive behavioral therapy, Stress management, Breast cancer, Quality of life (QOL)
Full-Text [PDF 684 kb]
(548 Downloads)
| Abstract (HTML) (1495 Views)
Full-Text: (568 Views)
Introduction
Breast cancer is a condition where cells in breast tissue grow abnormally [1]. It is currently the leading cause of death in women worldwide [2]. In Iran, breast cancer is also prevalent among women, especially in those aged 40-50. Thanks to advancements in diagnosis and treatment, the survival rate of patients with breast cancer has increased. Five-year and ten-year breast cancer survival rates are 90% and 80%, respectively. However, the survivors have to cope with the physical and psychological effects of their disease and treatment [3]. Patients with breast cancer have a poor quality of life (QOL). The QOL refers to the level of satisfaction with physical, emotional, and social abilities. It is crucial to identify the factors related to the QOL and better understand the health status of patients with chronic diseases. Patients with breast cancer have a poor QOL. In this regard, the QOL of cancer patients has become the primary focus of care in the field of oncology [4]. Among the common treatment methods for breast cancer, chemotherapy has a more negative effect on the QOL of patients. It disrupts physical, mental, social, and spiritual health, leading to reduced QOL [5].
Cancer evaluation and treatment can be very stressful, leading to the emergence of psychological symptoms that can exacerbate the disease, prolong the recovery process, and reduce the well-being of patients and their caregivers [6]. A variety of individual and environmental factors influences the perception of a stressful situation. These factors include the person’s thoughts, attitudes, and past experiences, all contributing to their overall perception of the situation. This, in turn, can lead to a range of physical, cognitive, and behavioral symptoms [7]. Cognitive-behavioral stress management (CBSM) therapy is a type of stress management method that is based on cognitive-behavioral therapy (CBT) and was developed by Beck [8] and Ellis [9] and to help people develop skills to reduce stress and cope more effectively with stressful situations [10]. The CBSM involves a range of techniques, such as increasing awareness of stress, learning relaxation skills, identifying unhelpful thoughts, restructuring cognitive processes, problem-solving training, building effective coping mechanisms, anger management, and improving self-expression [11].
Several studies have focused on the QOL of women with breast cancer. These studies have evaluated the effectiveness of various psychosocial interventions aimed at improving their QOL. Some of these interventions include written exposure therapy, mindfulness-based stress reduction [12], acceptance and commitment therapy [13], 5A model-based self-management program [14], and emotion-focused therapy [15]. Two systematic reviews of randomized controlled trials on the effect of CBT on the QOL of patients with breast cancer [4] and non-metastatic breast cancer [15] showed that the impact of CBT on the QOL of patients with breast cancer was moderate. However, there are contradictory results about the effect of cognitive-behavioral interventions on the QOL of women with breast cancer.
While there are several national and international studies on the efficts of cognitive-behavioral interventions on the QOL, including CBSM, this is the first study that was conducted in Mazandaran Province of Iran. The cultural and social context can have a significant impact on the QOL. This study aims to assess the effectiveness of CBSM therapy in improving the QOL of women with breast cancer in Sari, Iran.
Materials and Methods
This is an open-label randomized controlled clinical trial with a pre-test/post-test/follow-up design The study population consists of all women at early stages (stage 1-2) of breast cancer aged 30-50 years referring to Imam Khomeini Hospital and Baghban Clinic in Sari City. The sample size was determined 24 using G*Power software, version 301 at a 95% confidence interval (CI) and a test power of 80% according to a previous study [16]. Thirty samples were selected using non random available sampling and based on the entry and exit criteria and randomly divided into two groups of intervention and control. Seven women (out of 30), including three women from the intervention group (due to frequent absences) and two women from the control group (due to noncooperation), were excluded from the study. Therefore, the study was performed on 12 women in the intervention group and 13 in the control group.
The criteria for entering the study included age 30-50 years, non-metastatic breast cancer (stages 1-2), mastectomy surgery, 6-12 months have passed since the surgery, and consent to participate in the study. The exclusion criteria were unwillingness to continue participation in the sessions, having a mental disorder, absence from more than two intervention sessions, recurrence of the disease and suffering from a physical disease during the intervention.
The data collection tools were a demographic form and the short form of the World Health Organization QOL scale (WHOQOL-BREF), which is a 26-item tool and has four subscales (physical health, psychological health, social relationships, and environment) and one general scale (general health). The items are rated on a Likert scale from 1 to 5. The total score ranged 7-35 for physical health, 6-30 for psychological health, 3-15 for social relationships, 8-40 for environment and 2-10 for general health. Nejat et al. [17] translated this scale into Persian and reported its acceptable validity and reliability (Cronbach’s α=0.84). Also, the factor analysis approved the four-factor structure of the scale. Also, a study was conducted on 1167 people with chronic and non-chronic patients in Tehran using this scale. Test-re-test reliability for the subscales was reported as follows: 0.77 for physical health, 0.77 for psychological health, 0.75 for social relationships, and 0.84 for environment.
After obtaining ethical approval from the university and informed consent from the participants, both groups completed the WHOQOL-BREF. Then, group CBSM therapy was conducted in the intervention group at ten sessions of 120 minutes based on Antoni’s protocol translated into Persian by Safarzadeh et al. [18], in the conference room of Imam Khomeini Hospital in Sari. The post-test assessments were conducted immediately and one month after the end of the intervention. In similar studies, follow-up were conducted after one month [19], two months [18] and six months [20]. In this study, one month was determined because some women would finish the challenging course of chemotherapy after one month, and the subsequent changes could affect the results. Table 1 presents the protocol of the CBSM therapy.
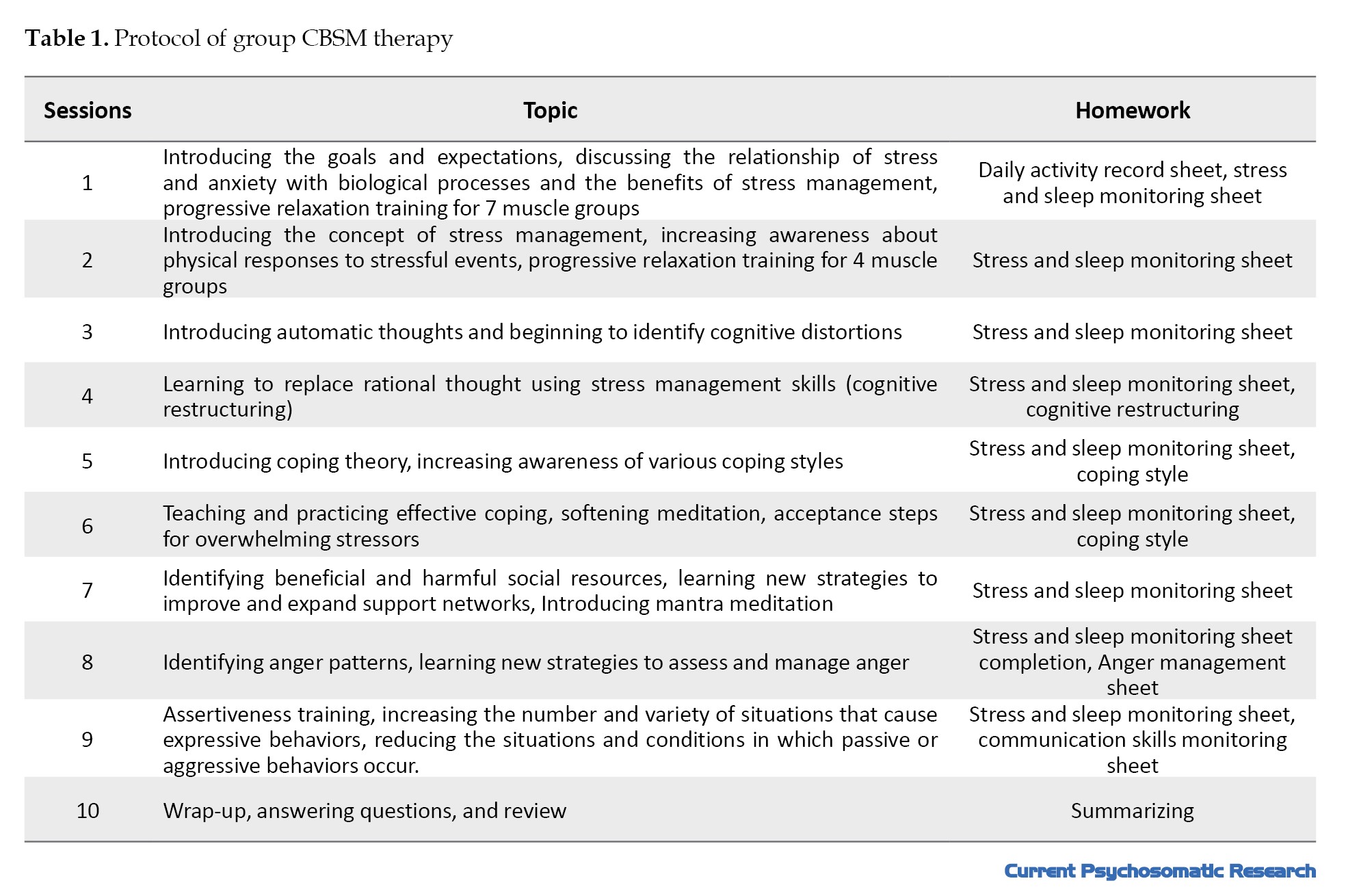
In all sessions, there was both behavioral intervention (relaxation) and cognitive training, but in the first two sessions, progressive muscle relaxation was also taught, and the subsequent sessions, started with relaxation exercises.
Statistical analysis
Descriptive and inferential statistics methods were used for data analysis in SPSS software, version 26. The significant level was set at 0.05. Repeated measures analysis of variance (ANOVA) followed by Bonferroni post hoc test for pairwise comparison was used for data analysis. Before conducting the analysis, Mauchly’s test of sphericity for assumption of sphericity, Kolmogorov-Smirnov and Shapiro-Wilk tests for the normality of the data, and Levene’s for assumption of equality of variances were conductd. The Kolmogorov Smirnov and Shapiro-Wilk tests confirmed the normality of the data. Levene’s test also confirmed the equality of variances in two groups (P˃0.05). However, the assumption of sphericity was not confirmed by Mauchly’s test for the QOL variable (P<0.001). Therefore, Greenhouse-Geisser correction was used to report the F ratio.
Results
There was no significant difference between the two groups in demographic characteristics according to the results of chi-square test reported in Table 2 (P˃0.05).
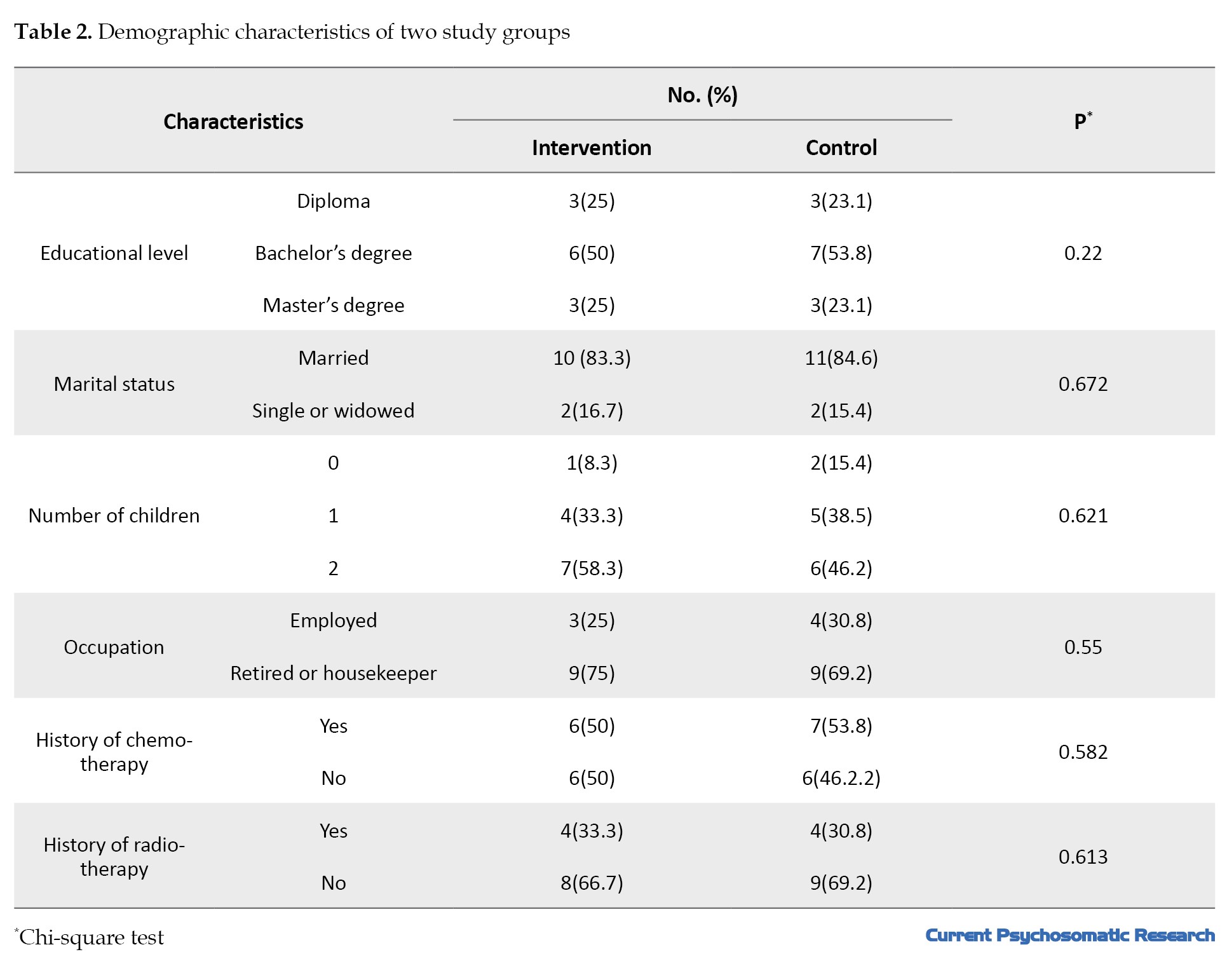
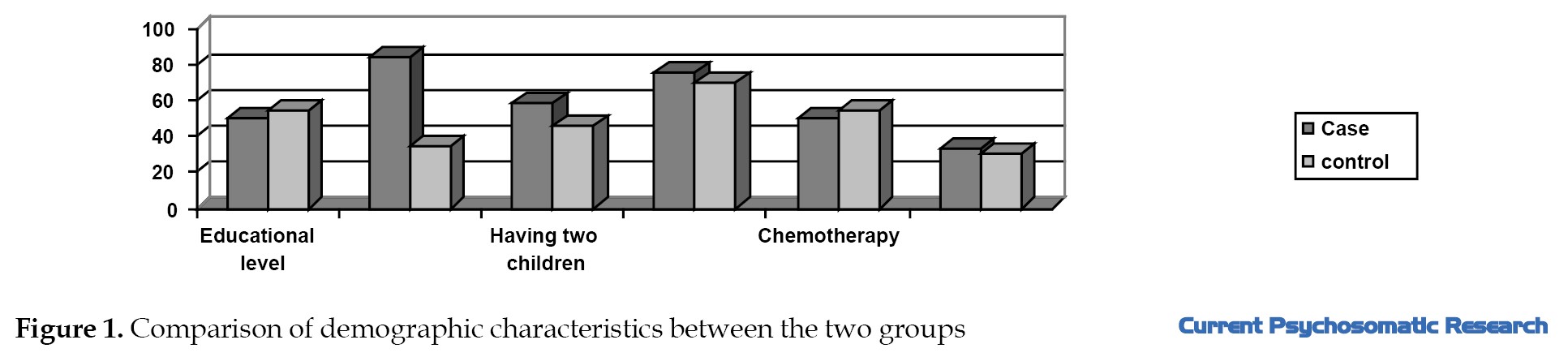
In terms of age, no significant difference was reported between the two groups, either (P=0.971). The mean age in both groups was about 44 years, ranged 30 to 50 years. The age range in the intervention group was 32-50 years, while in the control group, it was 34-50 years. Most of the participants were housekeepers and had two children. In terms of the type of treatment received after surgery, 50% had chemotherapy and 33.3% had radiation therapy in the intervention group. These percentages in the control group were 53.8% and 30.8%, respectively (P˃0.05). Figure 1 compares the two groups in terms of demographic characteristics.
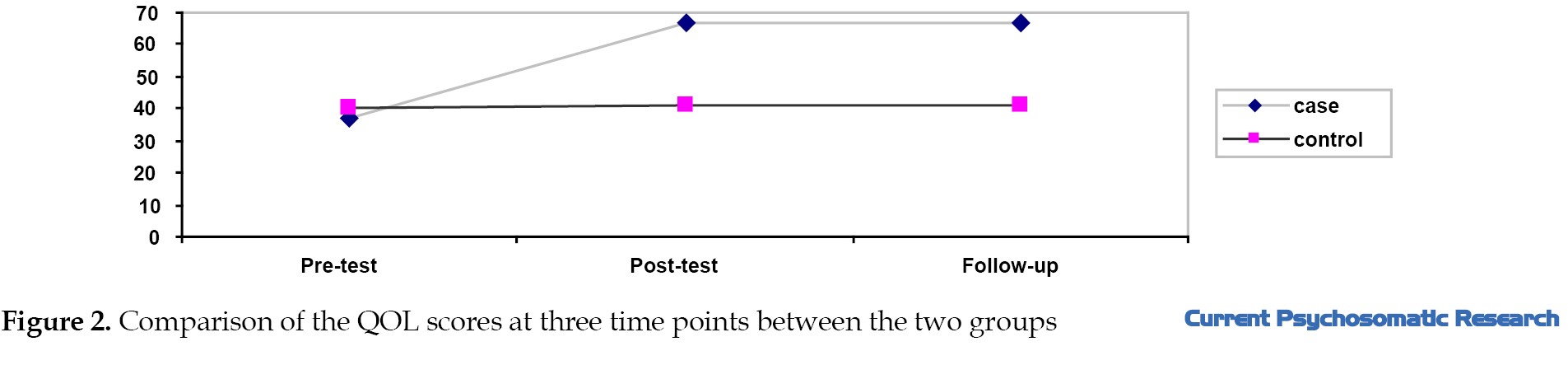
 As shown in Table 3, the mean score of the QOL in the pre-test phase in both control and experimental groups is very close to each other.
As shown in Table 3, the mean score of the QOL in the pre-test phase in both control and experimental groups is very close to each other.
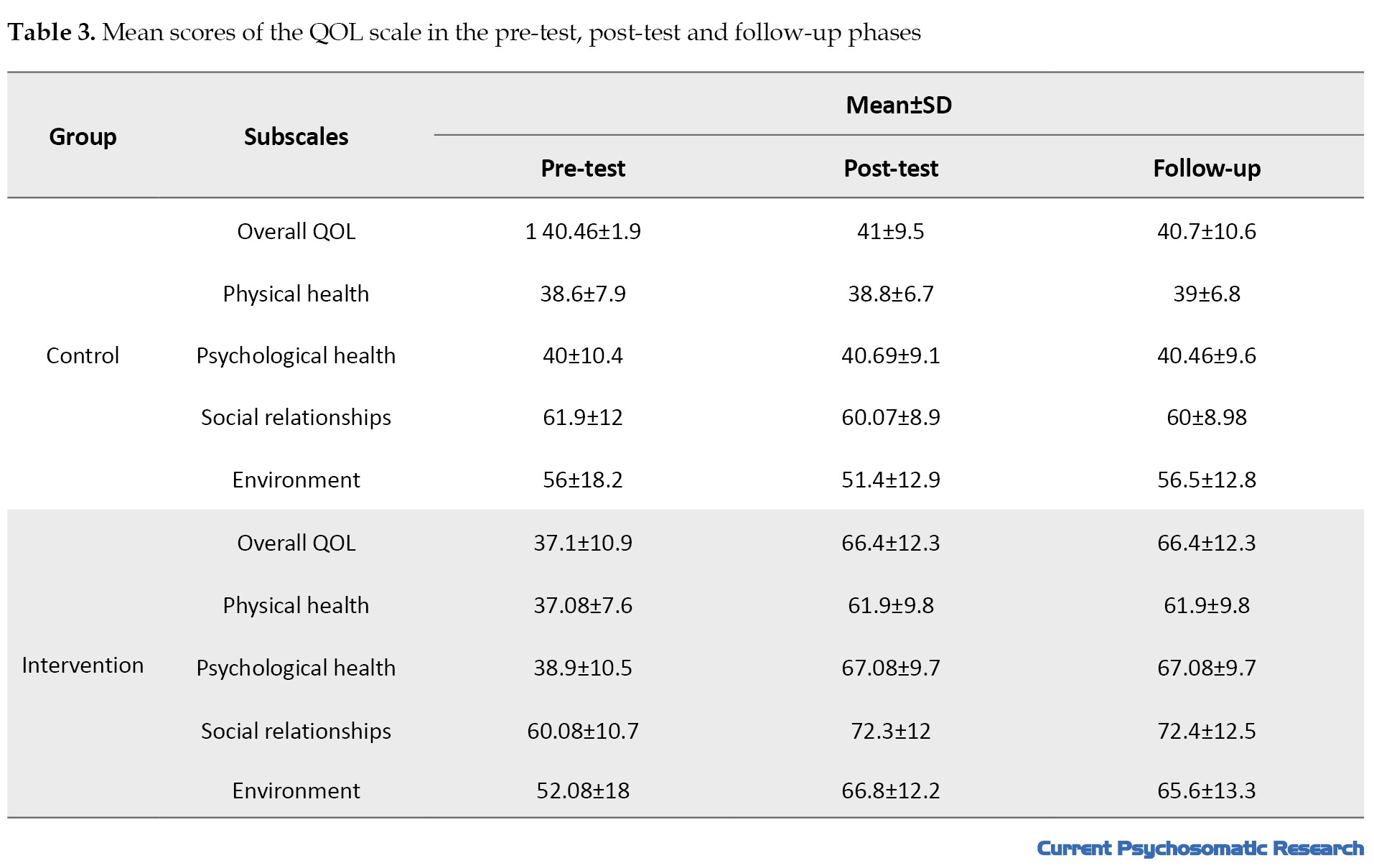
In the post-test and follow-up phases, there were considerable differences between the two groups, which are illustrated in Figure 2.
 According to the results of repeated measures ANOVA shown in Table 4, the F value for the effect of time (pre-test, post-test and follow-up) was statistically significant (P≤0.01).
According to the results of repeated measures ANOVA shown in Table 4, the F value for the effect of time (pre-test, post-test and follow-up) was statistically significant (P≤0.01).
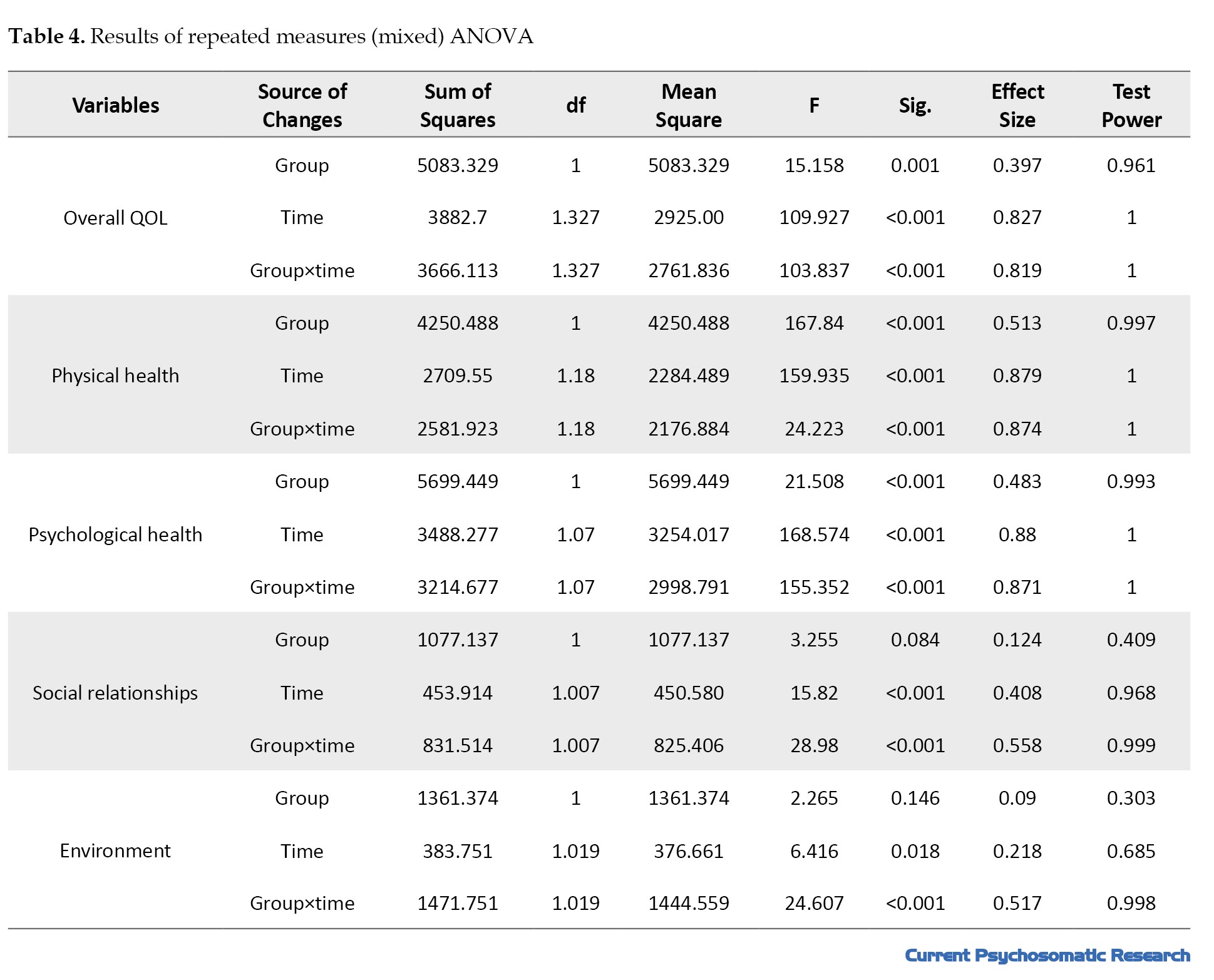
The interaction effect of time and group was also significant. Therefore, there was a significant difference in the mean scores of QOL over time.
The Bonferroni post hoc test was used to investigate the difference in the means between three time points. As shown in Table 5, the differences between the post-test and pre-test scores in the intervention group were higher and significant (P≤0.05), which indicates the effectiveness of CBSM therapy.
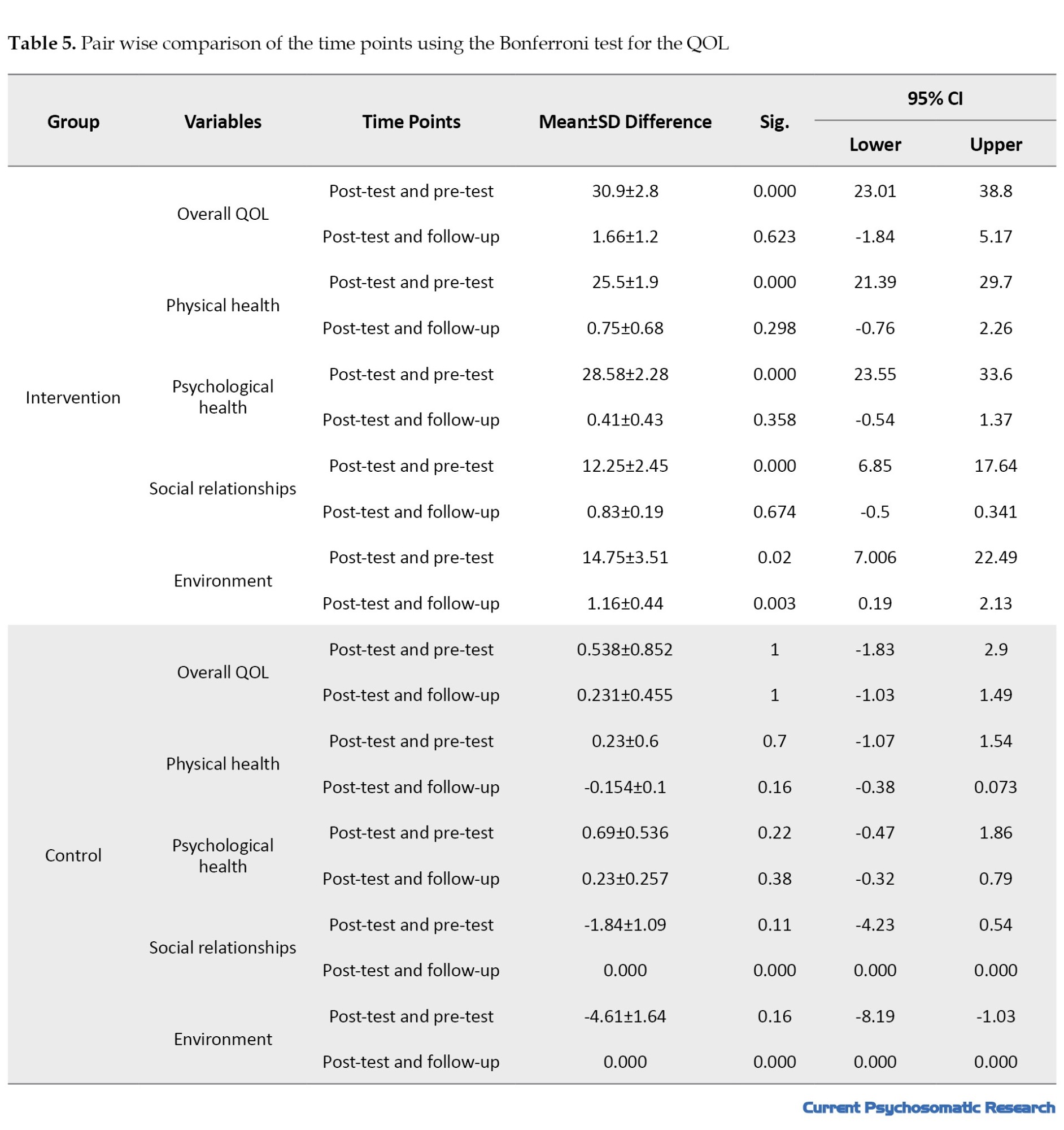
The differences between the post-test and follow-up scores in the intervention group were not significant (P˃0.05), indicating that the effect was maintained for one month. There was no significant difference between any time points in the control group.
Discussion
In this study, we found that the group CBSM therapy significantly increased the QOL scores of the intervention group. Therefore, it can be said that CBSM therapy is effective in improving the QOL of women with breast cancer. This is consistent with the results of Safarzadeh et al. [18], Getu et al. [4], Mohammadizadeh et al. [13], Habibi et al. [21], Shayan et al. [22], Rezaei Ardani et al. [23], Mohammadi Arya et al. [24] and Antoni et al. [25].
The intervention protocol was adapted from Antoni et al.’s study [20] and the QOL was measured by the WHOQOL-BREF. In other studies on the effect of CBSM on the QOL of breast cancer patients, different tools were used including the 12-item short form survey [21]; EORTC core QOL questionnaire (QLQ-C30) [18] and 36-item short form survey [24-26]. In one study [11], although the same tool was used for measuring QOL, the protocol was different from that of the present study. Also, in most of the related studies, the age range of participants was 20-60 years, while the age range was 30-50 years in our research.
In two systematic review studies on patients with breast cancer [4] and non-metastatic breast cancer [15], the effect of CBT on the QOL was reported to be moderate. However, this study showed that the CBSM therapy had a significant effect on the QOL of women with breast cancer. To explain the findings, it can be said that in the CBSM therapy, patients are taught to identify their sources of stress, evaluate and distinguish between positive and negative thoughts, identify the cause of these thoughts, and replace negative thoughts with rational thoughts. Also, emotional symptoms are managed by relaxation techniques. Therefore, by increasing the patients’ awareness of their thoughts and their connection with stress, it leads to reduced stress and thus improved QOL in various dimensions, especially physical and mental health.
Following the diagnosis of breast cancer, women suffer from various concerns, such as fear of death, worry about the treatment process and negative effect on appearance, the ability to perform daily tasks, and marital relations, and worry about its recurrence. Most of these women are in the age range of 40-50 years. In this age range, women are engaged in many family and social roles; therefore, breast cancer and its common treatments affect different aspects of the QOL [26]. By the CBSM, the stress can be managed step by step with relaxation training, and the underlying thoughts that cause stress are controlled by cognitive-behavioral methods, including paying attention to automatic thoughts, cognitive restructuring, assertiveness training, and learning effective ways to receive social support.
Conclusion
The CBSM can improve the QOL of women with breast cancer, and this effect can be maintained for one month. It can play an essential role in the treatment of breast cancer patients. It is recommended to conduct long-term studies using longer follow-up periods in the future. Also, it is recommended that future studies use a single-subject or qualitative design (based on the grounded theory using semi-structured interviews) to investigate the effectiveness of CBSM. The CBSM workshops for obstetrics and gynecology specialists and oncologists can be beneficial for providing quality care to women.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Sari Branch (Code: IR.IAU.SARI.REC.1402.047).
Funding
The article was extracted from the master's thesis of Fatemeh Toghani, approved by Department of Clinical Psychology, Faculty of Medicine, Islamic Azad University, Sari Branch.
Authors' contributions
Investigation and writing the initial draft: Fatemeh Toghani; Supervision, project administration, review and editing: Bahram Mirzaian and Ehsan Zaboli;Statistical analysis: Farzaneh Amin; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the staff of Imam Khomeini Hospital and Baghban Clinic in Sari and all the women participated in this study for their cooperation in this study.
References
Breast cancer is a condition where cells in breast tissue grow abnormally [1]. It is currently the leading cause of death in women worldwide [2]. In Iran, breast cancer is also prevalent among women, especially in those aged 40-50. Thanks to advancements in diagnosis and treatment, the survival rate of patients with breast cancer has increased. Five-year and ten-year breast cancer survival rates are 90% and 80%, respectively. However, the survivors have to cope with the physical and psychological effects of their disease and treatment [3]. Patients with breast cancer have a poor quality of life (QOL). The QOL refers to the level of satisfaction with physical, emotional, and social abilities. It is crucial to identify the factors related to the QOL and better understand the health status of patients with chronic diseases. Patients with breast cancer have a poor QOL. In this regard, the QOL of cancer patients has become the primary focus of care in the field of oncology [4]. Among the common treatment methods for breast cancer, chemotherapy has a more negative effect on the QOL of patients. It disrupts physical, mental, social, and spiritual health, leading to reduced QOL [5].
Cancer evaluation and treatment can be very stressful, leading to the emergence of psychological symptoms that can exacerbate the disease, prolong the recovery process, and reduce the well-being of patients and their caregivers [6]. A variety of individual and environmental factors influences the perception of a stressful situation. These factors include the person’s thoughts, attitudes, and past experiences, all contributing to their overall perception of the situation. This, in turn, can lead to a range of physical, cognitive, and behavioral symptoms [7]. Cognitive-behavioral stress management (CBSM) therapy is a type of stress management method that is based on cognitive-behavioral therapy (CBT) and was developed by Beck [8] and Ellis [9] and to help people develop skills to reduce stress and cope more effectively with stressful situations [10]. The CBSM involves a range of techniques, such as increasing awareness of stress, learning relaxation skills, identifying unhelpful thoughts, restructuring cognitive processes, problem-solving training, building effective coping mechanisms, anger management, and improving self-expression [11].
Several studies have focused on the QOL of women with breast cancer. These studies have evaluated the effectiveness of various psychosocial interventions aimed at improving their QOL. Some of these interventions include written exposure therapy, mindfulness-based stress reduction [12], acceptance and commitment therapy [13], 5A model-based self-management program [14], and emotion-focused therapy [15]. Two systematic reviews of randomized controlled trials on the effect of CBT on the QOL of patients with breast cancer [4] and non-metastatic breast cancer [15] showed that the impact of CBT on the QOL of patients with breast cancer was moderate. However, there are contradictory results about the effect of cognitive-behavioral interventions on the QOL of women with breast cancer.
While there are several national and international studies on the efficts of cognitive-behavioral interventions on the QOL, including CBSM, this is the first study that was conducted in Mazandaran Province of Iran. The cultural and social context can have a significant impact on the QOL. This study aims to assess the effectiveness of CBSM therapy in improving the QOL of women with breast cancer in Sari, Iran.
Materials and Methods
This is an open-label randomized controlled clinical trial with a pre-test/post-test/follow-up design The study population consists of all women at early stages (stage 1-2) of breast cancer aged 30-50 years referring to Imam Khomeini Hospital and Baghban Clinic in Sari City. The sample size was determined 24 using G*Power software, version 301 at a 95% confidence interval (CI) and a test power of 80% according to a previous study [16]. Thirty samples were selected using non random available sampling and based on the entry and exit criteria and randomly divided into two groups of intervention and control. Seven women (out of 30), including three women from the intervention group (due to frequent absences) and two women from the control group (due to noncooperation), were excluded from the study. Therefore, the study was performed on 12 women in the intervention group and 13 in the control group.
The criteria for entering the study included age 30-50 years, non-metastatic breast cancer (stages 1-2), mastectomy surgery, 6-12 months have passed since the surgery, and consent to participate in the study. The exclusion criteria were unwillingness to continue participation in the sessions, having a mental disorder, absence from more than two intervention sessions, recurrence of the disease and suffering from a physical disease during the intervention.
The data collection tools were a demographic form and the short form of the World Health Organization QOL scale (WHOQOL-BREF), which is a 26-item tool and has four subscales (physical health, psychological health, social relationships, and environment) and one general scale (general health). The items are rated on a Likert scale from 1 to 5. The total score ranged 7-35 for physical health, 6-30 for psychological health, 3-15 for social relationships, 8-40 for environment and 2-10 for general health. Nejat et al. [17] translated this scale into Persian and reported its acceptable validity and reliability (Cronbach’s α=0.84). Also, the factor analysis approved the four-factor structure of the scale. Also, a study was conducted on 1167 people with chronic and non-chronic patients in Tehran using this scale. Test-re-test reliability for the subscales was reported as follows: 0.77 for physical health, 0.77 for psychological health, 0.75 for social relationships, and 0.84 for environment.
After obtaining ethical approval from the university and informed consent from the participants, both groups completed the WHOQOL-BREF. Then, group CBSM therapy was conducted in the intervention group at ten sessions of 120 minutes based on Antoni’s protocol translated into Persian by Safarzadeh et al. [18], in the conference room of Imam Khomeini Hospital in Sari. The post-test assessments were conducted immediately and one month after the end of the intervention. In similar studies, follow-up were conducted after one month [19], two months [18] and six months [20]. In this study, one month was determined because some women would finish the challenging course of chemotherapy after one month, and the subsequent changes could affect the results. Table 1 presents the protocol of the CBSM therapy.
In all sessions, there was both behavioral intervention (relaxation) and cognitive training, but in the first two sessions, progressive muscle relaxation was also taught, and the subsequent sessions, started with relaxation exercises.
Statistical analysis
Descriptive and inferential statistics methods were used for data analysis in SPSS software, version 26. The significant level was set at 0.05. Repeated measures analysis of variance (ANOVA) followed by Bonferroni post hoc test for pairwise comparison was used for data analysis. Before conducting the analysis, Mauchly’s test of sphericity for assumption of sphericity, Kolmogorov-Smirnov and Shapiro-Wilk tests for the normality of the data, and Levene’s for assumption of equality of variances were conductd. The Kolmogorov Smirnov and Shapiro-Wilk tests confirmed the normality of the data. Levene’s test also confirmed the equality of variances in two groups (P˃0.05). However, the assumption of sphericity was not confirmed by Mauchly’s test for the QOL variable (P<0.001). Therefore, Greenhouse-Geisser correction was used to report the F ratio.
Results
There was no significant difference between the two groups in demographic characteristics according to the results of chi-square test reported in Table 2 (P˃0.05).
In terms of age, no significant difference was reported between the two groups, either (P=0.971). The mean age in both groups was about 44 years, ranged 30 to 50 years. The age range in the intervention group was 32-50 years, while in the control group, it was 34-50 years. Most of the participants were housekeepers and had two children. In terms of the type of treatment received after surgery, 50% had chemotherapy and 33.3% had radiation therapy in the intervention group. These percentages in the control group were 53.8% and 30.8%, respectively (P˃0.05). Figure 1 compares the two groups in terms of demographic characteristics.
In the post-test and follow-up phases, there were considerable differences between the two groups, which are illustrated in Figure 2.
The interaction effect of time and group was also significant. Therefore, there was a significant difference in the mean scores of QOL over time.
The Bonferroni post hoc test was used to investigate the difference in the means between three time points. As shown in Table 5, the differences between the post-test and pre-test scores in the intervention group were higher and significant (P≤0.05), which indicates the effectiveness of CBSM therapy.
The differences between the post-test and follow-up scores in the intervention group were not significant (P˃0.05), indicating that the effect was maintained for one month. There was no significant difference between any time points in the control group.
Discussion
In this study, we found that the group CBSM therapy significantly increased the QOL scores of the intervention group. Therefore, it can be said that CBSM therapy is effective in improving the QOL of women with breast cancer. This is consistent with the results of Safarzadeh et al. [18], Getu et al. [4], Mohammadizadeh et al. [13], Habibi et al. [21], Shayan et al. [22], Rezaei Ardani et al. [23], Mohammadi Arya et al. [24] and Antoni et al. [25].
The intervention protocol was adapted from Antoni et al.’s study [20] and the QOL was measured by the WHOQOL-BREF. In other studies on the effect of CBSM on the QOL of breast cancer patients, different tools were used including the 12-item short form survey [21]; EORTC core QOL questionnaire (QLQ-C30) [18] and 36-item short form survey [24-26]. In one study [11], although the same tool was used for measuring QOL, the protocol was different from that of the present study. Also, in most of the related studies, the age range of participants was 20-60 years, while the age range was 30-50 years in our research.
In two systematic review studies on patients with breast cancer [4] and non-metastatic breast cancer [15], the effect of CBT on the QOL was reported to be moderate. However, this study showed that the CBSM therapy had a significant effect on the QOL of women with breast cancer. To explain the findings, it can be said that in the CBSM therapy, patients are taught to identify their sources of stress, evaluate and distinguish between positive and negative thoughts, identify the cause of these thoughts, and replace negative thoughts with rational thoughts. Also, emotional symptoms are managed by relaxation techniques. Therefore, by increasing the patients’ awareness of their thoughts and their connection with stress, it leads to reduced stress and thus improved QOL in various dimensions, especially physical and mental health.
Following the diagnosis of breast cancer, women suffer from various concerns, such as fear of death, worry about the treatment process and negative effect on appearance, the ability to perform daily tasks, and marital relations, and worry about its recurrence. Most of these women are in the age range of 40-50 years. In this age range, women are engaged in many family and social roles; therefore, breast cancer and its common treatments affect different aspects of the QOL [26]. By the CBSM, the stress can be managed step by step with relaxation training, and the underlying thoughts that cause stress are controlled by cognitive-behavioral methods, including paying attention to automatic thoughts, cognitive restructuring, assertiveness training, and learning effective ways to receive social support.
Conclusion
The CBSM can improve the QOL of women with breast cancer, and this effect can be maintained for one month. It can play an essential role in the treatment of breast cancer patients. It is recommended to conduct long-term studies using longer follow-up periods in the future. Also, it is recommended that future studies use a single-subject or qualitative design (based on the grounded theory using semi-structured interviews) to investigate the effectiveness of CBSM. The CBSM workshops for obstetrics and gynecology specialists and oncologists can be beneficial for providing quality care to women.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Sari Branch (Code: IR.IAU.SARI.REC.1402.047).
Funding
The article was extracted from the master's thesis of Fatemeh Toghani, approved by Department of Clinical Psychology, Faculty of Medicine, Islamic Azad University, Sari Branch.
Authors' contributions
Investigation and writing the initial draft: Fatemeh Toghani; Supervision, project administration, review and editing: Bahram Mirzaian and Ehsan Zaboli;Statistical analysis: Farzaneh Amin; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the staff of Imam Khomeini Hospital and Baghban Clinic in Sari and all the women participated in this study for their cooperation in this study.
References
- Rehman S, Munawar N. Self-esteem, psychological wellbeing and locus of control among breast cancer patients. Pak J Humanit Soc Sci Res. 2022; 5(1):55-71. [DOI:10.32604/oncologie.2022.027640]
- Shang C, Xu D. Epidemiology of breast cancer. Oncologie. 2022; 24(4): 649-63. [DOI:10.32604/oncologie.2022.027640]
- Miller KD, Nogueira L, Devasia T, Mariotto AB, Yabroff KR, Jemal A, et al. Cancer treatment and survivorship statistics, 2022. CA Cancer J Clin. 2022; 72(5):409-36. [DOI:10.3322/caac.21731] [PMID]
- Getu MA, Chen C, Panpan W, Mboineki JF, Dhakal K, Du R. The effect of cognitive behavioral therapy on the QOL of breast cancer patients: A systematic review and meta-analysis of randomized controlled trials. Life Res. 2021; 30(2):367-84. [DOI:10.1007/s11136-020-02665-5] [PMID]
- Javan Biparva A, Raoofi S, Rafiei S, Pashazadeh Kan F, Kazerooni M, Bagheribayati F, et al. Global quality of life in breast cancer: Systematic review and meta-analysis. BMJ Support Palliat Care. 2024; 13(e3):e528-36. [DOI:10.1136/bmjspcare-2022-003642] [PMID]
- Emami M, Askarizade G, Faziltpour M. [Effectiveness of cognitive-behavioral stress management group therapy on resilience and hope in women with breast cancer (Persian)]. Positive Psychol Res. 2018; 3(4):1-14. [DOI:10.22108/ppls.2018.106094.1217]
- Diaz A, Taub CJ, Lippman ME, Antoni MH, Blomberg BB. Effects of brief stress management interventions on distress and leukocyte nuclear factor kappa B expression during primary treatment for breast cancer: A randomized trial. Psychoneuroendocrinology. 2021; 126:105163. [DOI:10.1016/j.psyneuen.2021.105163] [PMID]
- Beck AT. Cognitive approaches to stress. Principles and practice of stress management. 1984. [Link]
- Ellis A. The future of cognitive behavior and rational emotive behavior therapy. In: Carlson J, Knaus W, editor. Albert Ellis Revisited. New York: Routledge; 2013. [Link]
- Urizar Jr GG. Stress and cortisol regulation during pregnancy: Implications for cognitive behavioral stress management among low-income women. In: Martin CR, Patel VB, Preedy VR, editors. Handbook of lifespan cognitive behavioral therapy. Amsterdam: ScienceDirect; 2023. [DOI:10.1016/B978-0-323-85757-4.00034-1]
- Ahmadian H, Ghaderyan A, Abdi M. [The effectiveness of cognitive behavioral stress management training on anxiety and blood pressure control in hypertensive men (Persian)]. Med J Mashhad Univ Med Sci. 2022; 65(3):1082-91. [DOI:10.22038/mjms.2022.44844.2573]
- Shalikari M, Mirzaian B, Abbasi G. [Effect of written exposure therapy (WET) Vs. mindfulness-based stress reduction (MBSR) on managing pain and mental adjustment to cancer in women with breast cancer (Persian)]. J Nurs Manage Orginal Article. 2023; 12(1):31-48. [Link]
- Mohammadizadeh S, Khalatbari J, Ahadi H, Hatami HR. [Effectiveness of acceptance and commitment therapy on perceived stress, body image and QOL in women with breast cancer (Persian)]. Sci J Soc Psychol. 2021; 9(57):87-100. [DOI:10.32598/hsmej.10.1.417]
- Kalhor M, Fathi M, Ghaderi B, Roshani D, Ozairi S, Rashidi K. [Effect of five a model self-management on QOL in patients with breast cancer. Avicenna J Nurs Midwifery Care (Persian)]. 2019; 27(4):269-80. [DOI:10.30699/ajnmc.27.4.269]
- Jassim GA, Doherty S, Whitford DL, Khashan AS. Psychological interventions for women with non-metastatic breast cancer. Cochrane Database Syst Rev. 2023; 1(1):CD008729. [DOI:10.1002/14651858.CD008729.pub3] [PMID]
- Jamilian H, Ghafouriasar S, Bayat A. Effectiveness of cognitive-behavior stress management on reducing clinical symptoms in patients with breast cancer. Payesh. 2021; 20(2):201-11. [DOI:10.52547/payesh.20.2.201]
- Nejat SA, Montazeri A, Holakouie Naieni K, Mohammad KA, Majdzadeh SR. [The World Health Organization quality of Life (WHOQOL-BREF) questionnaire: Translation and validation study of the Iranian version (Persian)]. J Sch Public Health Inst Public Health Res. 2006; 4(4):1-2. [Link]
- Safarzade A, Roshan R, Shams J. Effectiveness of stress management and relaxation training in reducing the negative affect and in improving the life quality of women with breast cancer. J Res Psychol Health. 2013; 6(4):21-35. [Link]
- Dodds SE, Pace TW, Bell ML, Fiero M, Negi LT, Raison CL, et al. Feasibility of cognitively-based compassion training (CBCT) for breast cancer survivors: A randomized, wait list controlled pilot study. Supportive Care Cancer. 2015; 23:3599-608. [DOI:10.1007/s00520-015-2888-1]
- Antoni MH, Lechner S, Diaz A, Vargas S, Holley H, Phillips K, et al. Cognitive behavioral stress management effects on psychosocial and physiological adaptation in women undergoing treatment for breast cancer. Brain Behav Immun. 2009; 23(5):580-91. [DOI:10.1016/j.bbi.2008.09.005] [PMID]
- Habibi J, Habibi M, Malekzade M, Ghanbari N. Effectiveness of cognitive-behavioral stress management on increasing QOL in patient with breast cancer. Res Clin Psychol Couns. 2017; 6(2):96-110. [DOI:10.18502/jzms.v5i1.10322]
- Shayan A, Refaei M, Jamshidi F. [Investigating the effect of cognitive-behavioral stress management on occupational performance among women with breast cancer (Persian)]. Curr Women’s Health Rev. 2020; 16(2):152-9. [DOI:10.22067/ijap.v6i2.33858]
- Rezaei Ardani A, Farid Hoseini F, Borhani Moghani M, Seyfi H. [Cognitive behavioral stress management effects on QOL and negative emotions in women with breast cancer (Persian)]. The Iran J Obstet Gynecol Infertil. 2015; 18(154):8-18. [DOI:10.22038/ijogi.2015.4718]
- Mohammadi Arya A, Pakdaman M, Abolghasemi S, Rezaee M, Pashaee T, Ghareh Tapeh A. The effect of stress inoculation group training on hope and QOL in women with breast cancer. J Res Dev Nurs Midwifery. 2014; 11(1):8-16. [Link]
- Antoni MH, Wimberly SR, Lechner SC, Kazi A, Sifre T, Urcuyo KR, et al. Reduction of cancer-specific thought intrusions and anxiety symptoms with a stress management intervention among women undergoing treatment for breast cancer. Am J Psychiatry. 2006; 163(10):1791-7. [DOI:10.1176/ajp.2006.163.10.1791] [PMID]
- Oers H, Schlebusch L. Indicators of psychological distress and body image disorders in female patients with breast cancer. J Mind Med Sci. 2020; 7(2):179-87. [DOI:10.22543/7674.72.P179187]
Type of Study: Research |
Subject:
Psychology
Received: 2022/07/5 | Accepted: 2023/10/29 | Published: 2024/01/1
Received: 2022/07/5 | Accepted: 2023/10/29 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Address: Mazandaran University of Medical Sciences, Moallem Square, Sari, Iran.
Journal Office Tel: +981134343407
Email: cpr mazums.ac.ir
mazums.ac.ir
Publisher: Negah Institute for Social Research & Scientific Communication
Publisher Tel: +9821 4535 5555; +9821 4535 5000
